
Morgellons : A Working Hypothesis
Neural, Thyroid, Liver, Oxygen, Protein and Iron Disruption
(Link to Parts I, II, III – Click Here)
PART III
POTENTIAL MITIGATING STRATEGIES (RESEARCH BASED)
Clifford E Carnicom
Dec 18 2013

Art work courtesy of David Dees with permission.
Note: I am not offering any medical advice or diagnosis with the presentation of this information. I am acting solely as an independent researcher providing the results of extended observation and analysis of unusual biological conditions that are evident. Each individual must work with their own health professional to establish any appropriate course of action and any health related comments in this paper are solely for informational purposes and they are from my own perspective.
This paper seeks to identify a host of organic compounds that are likely to comprise the core physical structure of biologically produced filaments characteristic of the Morgellons condition. A biological oral filament sample will be analyzed for the presence of candidate organic functional groups using the methods of infrared spectrophotometry. Potential health impacts from these same core structures are examined and compared to the observed , reported and documented symptoms (in part) of this same condition. Potential mitigating strategies, from a research perspective only, are discussed.
A body of evidence, accumulated over a period of several years, reveals that the Morgellons condition is likely characterized by a host of serious physiological and metabolic imbalances. These imbalances are caused by the disruption of a variety of major body processes including, as a minimum, the regulation of metabolism by the thyroid, potential liver enlargement, a decrease of oxygen in the circulatory system, the utilization of amino acids important to the body, the oxidation of iron and a potential impact to neural pathways. The impact of this degradation to human health can be concluded to be serious, debilitating and potentially lethal in the cumulative sense; the reports of those who suffer from the condition are in alignment with these conclusions. This paper will summarize the body of work and chronology which leads to this more comprehensive hypothesis.
The health, medical and governmental communities will again be invited to offer their expertise and contributions , as well as to assume their role of responsibility and the obligations of their professions to serve the public.
This paper will be divided into three phases:
I. Identification of the functional groups / components
II. Potential health impacts of the various functional groups identified.
III. Potential mitigating strategies (research-based)
PART III
POTENTIAL MITIGATING STRATEGIES (RESEARCH BASED)
We now begin the final phase of this paper, and this is to introduce, recall and compile a host of strategies and considerations that may be helpful to mitigate some of the impacts upon health by the Morgellons condition. Some of the work that has been done previously will also be incorporated into and repeated within this section; much of this work remains especially valuable and relevant here as well. It is important to understand that this information is derived from an individual research standpoint only, and that it does not represent any medical advice or diagnosis whatsoever. The usual disclaimer and caveat will be repeated before we begin the conversation:
|
Note: I am not offering any medical advice or diagnosis with the presentation of this information. I am acting solely as an independent researcher providing the results of extended observation and analysis of unusual biological conditions that are evident. Each individual must work with their own health professional to establish any appropriate course of action and any health related comments in this paper are solely for informational purposes and they are from my own perspective. |
Before we begin in earnest, it is worthwhile to examine the basic mechanisms of disease. In my own journey of study and discovery in the field of health and disease, it astounds me that these principles are actually so well established and yet they are often not understood and applied. There may be a fairly broad gap between what has been understood for some time and what the public is generally aware of with respect to disease; it is hopeful that this situation continues to improve. What especially interests me is that these principles exist irrespective of the particular condition or disease examined; we often think of each situation as being so unique and complex that we think that we can only make headway with advanced and specialized knowledge. This is not necessarily the case if we take the list that follows to heart. We find these “mechanisms” listed in the standard textbooks of pathology and, in particular, within the very first chapter of the well established tome entitled, Robbins Pathological Basis of Disease57, 4th Edition. It is succinctly stated that:
| “Although it is not always possible to determine the precise biochemical site of action of an injurious agent, four intracellular systems are particularly vulnerable:
(a) maintenance of the integrity of cell membranes (b) aerobic respiration (c) synthesis of enzymic and structural proteins and (d) preservation of the integrity of the genetic apparatus of the cell.” |
What we have been given here close to 25 years ago, if we care to address it, is the basis of disease in the body. The statement is not qualified with respect to what type of disease is taking place, it is the basis of disease itself. From my studies, I find no important exceptions to this as it applies to the so-called “Morgellons” condition.
We can all interpret this in our own light, but my rudimentary interpretation is that to remain healthy:
1. We must remain intact and structurally sound at a cellular level.
2. We must use oxygen efficiently and effectively in our bodies, as respiration is the source of all energy to the body.
3. We must continue to repair the actual structures of the body to compensate for decay and age.
4. We must be able to reproduce in a healthy fashion to flourish and prosper as a species.
This is the challenge that we must assume to combat disease or ill health, regardless of what the particular situation or circumstances are. It is no different here, at the most basic level of understanding, from the case of harm in general. Of course we seek to be specific as to how this is done under the specific plight of the Morgellons condition, but it is rather astounding how evident that course is when armed with the most rudimentary knowledge of pathology. Dr. Stanley Robbins will also get us off to a good start on this topic58, with his equally succinct listing of causative agents, such as physical agents, chemical agents and drugs, infectious agents, immune responses, genetic damage and nutritional imbalances. We should never miss this grand view before becoming engrossed in the detail.
I have spoken earlier to those that seek a simple pill in life to take care of the complexities that are before us; I am not your person to listen to for a myriad of reasons. My course of research is one that seeks the fundamental understanding of the situation and that seeks to make this information accessible to all. Remedies to problems as needed must, therefore, also be accessible to all – at least to the highest degree possible. Specialized drugs and technologies are under the purview of others with resources, means and motive. You must seek them elsewhere. The work of this Institute is to research and educate on behalf of the general welfare and public with the resources that the public makes available to us.
Keeping the above foundation in mind at all times, let us go to work on the specifics. It is helpful to have the master list that has evolved before us again. This list basically identifies potential causative agents or mechanisms in conjunction with potential heath impacts (either reported or research-based). This master list, as formulated, will have numerous overlaps and redundancies occurring between the two sets, and it is not to be viewed in a style of one-to-one correspondence. Let us see if we can make some headway after the table is reviewed again:
|
Candidate Functional Groups or Constituent Identified within the Biological Filaments: |
Reported, Observed or Research-Based Candidate Health Impacts or Symptoms of the Morgellons Condition: |
|
Iron Bacterial or Bacterial-Like (Chlamydia P. or Chlamydia P.-like) Repeating Structure within both Blood and Filaments Amino Acid Deficiency – in general Specific Amino Acid: Cysteine Specific Amino Acid : Histidine Amines Carboxylic Acids Aromatics Aromatic substituted Alkenes Aromatic substituted Amines Alkanes Aldehydes Phenols Alkyl Halides |
|
|
Oxygen deprivation;diminished oxygen carrying capacity of the blood |
|
|
Significant oral filament production; the presence of filament structures (ferric iron – anthocyanin complexes) within oral samples. (red wine test) |
|
|
|
|
|
Skin-borne filament production; skin manifestation at the more developed levels (the skin is an excretory organ). |
|
|
|
|
|
Extended or Chronic Fatigue |
|
|
Hair alterations, i.e., texture, thickness, loss of hair |
|
|
|
|
|
Gastro-intestinal imbalance |
|
|
Immune system breakdown |
|
|
The impact of increased oxidation, greater free radical presence and their damaging effects upon the body. |
|
|
|
|
|
Lower energy levels due to interference in the ATP production cycle; greater fatigue |
|
|
|
|
|
Any bacterial forms that infect the blood requires iron if it is to grow and reproduce. |
|
|
|
|
|
The smoking population may exhibit an increased incidence of the condition due to additional oxygen inhibition within the blood. |
|
|
|
|
|
Specific blood abnormalities |
|
|
|
|
|
Metabolic disruption |
|
|
|
|
|
Liver toxicity, gall bladder and bile duct complications. |
|
|
|
|
|
An increased level of acidity in the body. |
|
|
|
|
|
Skin lesions |
|
|
|
|
|
Chronic Decreased Body Temperature |
|
|
|
|
|
Neurological Impairment (e.g., blurred vision, slurred speech, ringing of ears (tinnitus), loss of coordination, loss of strength) |
|
|
|
|
|
Cognitive impairment, i.e., mental confusion, inability to concentrate, short term memory loss, “brain fog” |
|
|
|
|
|
Joint Pain |
|
|
|
|
|
Liver Toxicity |
|
|
|
|
|
Respiratory problems, including proclivities toward a chronic cough or walking pneumonia-like symptoms |
|
|
|
|
|
The presence of a bacterial-like component (chlamydia-like) within or surrounding the red blood cells |
|
|
|
|
|
Unusual or extreme dental issues; tooth decay or loss |
|
|
Chronic itching of the skin |
|
|
Associations between oxygen deprivation, glycolysis, anaerobic respiration, cancer, energy production (ATP), and intracellular acidity |
|
|
Research indicates the urinary tract may be equally affected with the presence of the filament structures |
On a macro scale, we can see that some of the more obvious issues to be addressed concern iron disruption, amino acid presence and protein rebuilding, acidity, oxidative stress, availability of oxygen, thyroid and metabolism issues, halogen toxicity and substitution concerns, joint and skeletal integrity and elasticity, blood and cellular integrity, and potential neural disruption. Unfortunately, the list is not exhaustive but it is representative of some of the health concerns that have been brought to the forefront and reported on.
One of the interesting prospects of mitigation is that improving a limited set of disrupting influences may have benefits that extend to the wider system of health. It might seem overwhelming to address such an array of problems, but the more that is understood between the relationships of mitigation, the greater are the chances of improvement to health on the whole. We must all start somewhere when we begin to assume greater responsibility for our awareness and state of health; this beginning can basically become a way of life rather than a fix to a singular problem.
Let’s begin with the iron problem, as it has been discussed extensively59,60,61 and it remains as a paramount issue. If it is accepted that iron interference is taking place, what course(s) of action might exist? Studying these previous papers, it can be seen that a fair deincreasing thegree of effort has already been extended to this question. It is appropriate to recall some of this information as follows:
1. ” Increasing the utilization and absorption of existing iron within the body. Iron is certainly one of the most important elements of the body. Referring to the Linus Pauling Institute,
One of the findings from the study of coordination chemistry described above is that iron has the ability to bond with numerous other molecules. For example, iron (in the Fe2+ state) preferentially bonds to oxygen. If the iron is altered to the Fe(3+) state. it will no longer bond to oxygen. In this modified state, the iron will then form additional bonds to other molecules, many of which are harmful as has also been described above. The idea of a chelator is to keep the oxygen bound in a protected state where it can not bind so easily with other, often harmful, molecules. Heme itself, within hemoglobin, is a classic example of a chelator. If our iron has been altered to where it becomes free or bound to other molecules (potentially harmful ligands), the solution to that problem would not seem to be to take more iron, any more than increasing the oxygen intake is expected to resolve a problem of oxidation. The more effective solution would appear to be to keep the iron in a chelated state, where it is bound and protected by the expected molecules and proteins such as heme in the body. This therefore suggests that increased attention would be devoted to the study and role of chelators in human health. It does not seem reasonable that we would automatically pursue a path of increasing iron intake; indeed this process can be quite harmful and dangerous to human health. Again, the importance of consultation with the medical professionals of choice is unequivocally stated; the stakes of the issues we are speaking of are of the highest importance. 2. The inhibition of the growth of iron-consuming bacteria (and bacteria-archea like) forms. We know now that the organism uses iron for its existence and growth. It appears that iron in the further oxidized state (i.e, Fe3+) is of primary benefit to the organism. We also know, in retrospect, that iron is a critical metabolic element within many of the bacteria (or bacteria-archaea like forms). One strategy that develops with such organism is that of inhibiting the ability of the organism to access or metabolize the iron. This once again brings up the idea of a chelator. This topic has also been discussed in an earlier paper, and introduced the role of human breast milk and its resistance to bacterial forms in infant growth96. Lactoferrin (found in whey) was identified as a potential strong chelating protein within that research. Transferrin is another protein chelator within the human digestive tract that serves a similar purpose, i.e., binding of the iron and consequently it becomes less accessible to iron-consuming bacteria (or bacteria-archea like forms).” |
We also recall from the earlier papers mentioned an important discussion about the potential benefits of Vitamin C, NAC (N-Acetyl Cysteine) and glutathione. These three compounds are powerful anti-oxidants and they also relate directly to the issue of oxidative stress in addition to that of iron disruption:
| “Three methods that appear to interfere with the molecular bonding of the iron-dipeptide complex that is now understood to be characteristic of the “Morgellons” growth structure have been established and identified. The iron-protein complex is believed to be of, or similar to, the “Rieske Protein” (iron-sulfur) form. These three methods also appear to be variably successful in reducing the oxidation state of the encapsulated iron from the Fe(III) state to the Fe(II) state. The discovered methods involve the use of ascorbic acid (Vitamin C), N-acetyl cysteine (NAC) and glutathione. The results of applying glutathione appear to be especially promising at this time, as it appears that a major disruption in the bond structure has taken place after approximately 72 hours. The methods have been established and verified through visual, chemical and spectroscopic methods and each has an effect independent of the others. The hypothesis to be made here is that the growth of the organism itself may be interfered with as a result of this work.“ |
The reader is advised to consult the Institute referenced papers for the detailed information that underlies the excerpts given:
A Carnicom Institute research discussion on this and related issues has also been made available to the public previously. In addition, a series of videos that discuss the importance of glutathione (and its precursors) has also been included within the earlier papers.
|
Listen to a Research Discussion on This Topic View A Series of Informational YouTube Videos on Glutathione |
The question of whether to take a supplement of iron or not will not be discussed here; this harkens to the pill philosophy discussed earlier. This question will not only apply to iron supplements, it will apply to any and all questions that will be addressed concerning supplements of any kind. I will report on the research facts available to us all; we must then assume our individual responsibilities of action or discussion with the health professionals and advisors of our choice. It is not my role or position to be involved in any individual concerns or requests. I am not acting in any medical capacity whatsoever; I am acting fully and completely as an independent researcher.
The importance of the honest and dedicated involvement of the health and medical communities should be obvious to all of us; I encourage you to force this issue as it deserves.
In the particular case of iron supplements, there are risk involved as with most to all things that human beings can ingest. Specifically, unwarranted iron consumption can lead to:
| “Iron supplements can cause indigestion, stomach pain, constipation, diarrhea, nausea, vomiting, back pain, muscle pain, chest pain, chills, lightheadedness and fainting, rapid heartbeat, fever, sweating, flushing, headache, metal taste, numbness or tingling in the hands and feet, rash and breathing problems62.” |
In the case of high dosages, it can:
| “High doses of iron can cause stomach and intestinal problems, liver failure, dangerously low blood pressure and death. Iron poisoning is the most common cause of poisoning deaths in children, according to Medline Plus. Symptoms of iron poisoning include bloody diarrhea, fever, nausea, sharp stomach pain and severe vomiting — possibly of blood — a blue tint to the lips, nails and palms, seizures, pale or clammy skin, shallow or rapid breathing, extreme fatigue and a weakened or fast heartbeat63.” |
Obviously, it would seem to be of greater interest to efficiently utilize existing iron within the body rather than to assume the addition of iron automatically addresses the problem. It has also been discussed in previous papers that Vitamin C (ascorbic acid), in addition to being a powerful antioxidant, helps to increase the absorption of iron into the body. From a current reference, we can see that there are two methods by which this occurs64:
1. Vitamin C (ascorbic acid) helps to prevent the formation of non-soluble iron forms.
2. Vitamin C reduces iron from the ferric (Fe3+) to the ferrous (Fe2+) state.
The importance of this latter statement must be emphasized again, and it is the very basis of the paper entitled “The Breaking of Bonds and the Reduction of Iron” presented in November of 201265.
| We can see, therefore, that iron in the ferrous (Fe2+) state is generally going to be more bio-available in the ferric state vs. in the ferric state, both from the standpoint of iron-oxygen binding in the blood as well as in the direct absorption of iron by mucosal cells. It has been shown in the laboratory through Institute research that vitamin C, NAC (N-acetyl cysteine) and glutathione have each been effective in this reduction process from the ferric to the ferrous state. It would be worthwhile to review the details of the Institute reference papers that have been cited in this report; the discussions related to glutathione and its precursors (as opposed to direct supplementation) are especially important (i.e., the use of NAC). |
| The roles of chelation as well as anti-oxidants, as they have been discussed, should also be given full consideration for their potential benefits prior to assuming supplementation is a logical strategy. |
Understanding the co-existence between iron and bacteria should also help in the process of setting priorities for healing. Also, from the earlier paper66:
| “A bacterium that infects the blood requires a source of iron if it is to grow and reproduce.”
“Like their human hosts, bacteria need iron to survive and they must obtain that iron from the environment. While humans obtain iron primarily through the food they eat, bacteria have evolved complex and diverse mechanisms to allow them access to iron… Iron is the single most important micronutrient bacteria need to survive… understanding how these bacteria survived within us is a critical element of learning how to defeat them”We may, therefore conclude that: The elimination of bacterial infections in the body would, therefore, obviously be beneficial in increasing the utilization of existing iron; additional iron via a supplement might simply act as a facilitating nutrient to detrimental bacterial forms. It is also of much interest to present within in this research that NAC (N-acetyl cysteine) has two additional benefits in addition to its effectiveness as an anti-oxidant. In the following paper by the pathologist David Wheldon it is clearly stated that NAC also68: 1. has the ability to destroy chlamydial elementary bodies. 2. replenishes intracellular glutathione. Those familiar with the research of this site will be aware of the extensive investigation and study that has been placed upon the “chlamydia-like” or “bacterial-like” form that has been repeatedly identified within the filament structures. The difficulties of eliminating that particular bacterial form have also been made apparent; hence the chronic respiratory symptoms that accompany its presence. The imperviousness of these “elementary bodies” (i.e, a spore-like form that remain dormant for extended periods) is at the heart of that difficulty. The use of NAC as an important precursor to the formation of glutathione (one of the most powerful anti-oxidants that exists) has also been previously discussed on this site. The many benefits of NAC (and also its reported anecdotal success with its use with Morgellons) can now be better understood with respect to its chemistry, its specific actions of reduction (anti-oxidation) and its precursive role in the formation of glutathione. It is also of clear and immediate interest that this same paper states that the mechanism of destruction of these elementary bodies is by the breaking of disulphide bonds within the chlamydia organism (see discussion immediately below). |
We now migrate to the amino acid – protein issue, and it becomes increasingly apparent that any separation of our topics is largely artificial. In addition to the withdrawal and diversion of iron from the body to support a parasitic life form, the redirection of amino acids and proteins to support such a life form is an equally serious matter. Proteins make up more than fifty-percent of our bodily constitution and they are made from amino acids; if these are interfered with in any fashion it is inevitably to our detriment. The research evidence does indicate that such interference is taking place. There are a minimum of three amino acids that exist at the top of the interest list, and it should not be surprising if there are others. The three of immediate interest include cysteine, histidine and tryrosine; again, there may well be others.
The original interest in cysteine emerged from the original observations of strength of the bonds of the filament materials, both environmental and biological. The materials, from the beginning, have shown tremendous resistance to chemical and physical agents, such as acids, alkalies and temperature. This indicates, from the onset, the likely existence of disulphide bonds, which are characteristic of both cysteine and cystine forms. Cysteine is an amino acid that is characterized by the presence of sulfur, which can then further form disulphide bonds. For example, hair is largely composed of keratin (a protein), and this protein is largely composed of such disulphide bonds. This is one reason that hair is similarly so resistant to chemical breakdown. The presence of cysteine with the filament forms (environmental and biological) has been further supported by direct observation via visible light spectrophotometry in combination with ninhydrin testing. The presence of amines (building blocks of amino acids) has been further confirmed with infra-red spectrophotometry described in this report.
The interest in histidine has also come about with the use of visible light spectrophotometry in combination with ninhydrin; please refer to the earlier paper entitled “Amino Acids Verified” for additional details of this earlier project67. This interest has also been extended with the knowledge of the existence of the histidine side chain in the heme (hemoglobin) molecule coupled with the observation of the extensive breakdown in the integrity of the red blood cells (erythrocytes). There is ample reason to focus on the likely existence of histidine (an amino acid) as a part of the biological filament growth form.
The interest in tryosine comes solely from the current work with IR spectrometry and the subsequent relationships that have been identified with both dopamine (a neuro-transmitter) and thyroxine (a primary metabolic hormone of the thyroid). Interest in this particular amino acid is also increased due to knowledge of some of the mechanisms of aromatic chemistry, particularly the substitution reactions involving the halogens and the hydroxyl groups. These have been discussed at length in this report and they both suggest the very real possibility of structural disturbances to both thyroxine and dopamine within the body. In addition, the observed symptoms of the Morgellons condition are primary data points in our study and must not be denied. The strong presence of metabolic, neural and cognitive interference in conjunction with the Morgellons condition gives, by itself, just cause to investigate any tyrosine disruptions that may be in place. The combination of all factors above, IR observations, aromatic chemistry and reported symptoms all lend themselves to a deep investigation of the tyrosine, thyroxine, dopamine and oxidopamine issues and relationships.
An additional interest regarding collagen, a protein, has also developed prominently over the this last year especially in relation to the issue of joint pains. Joint pains are another of the primary symptoms that are on record in association with the Morgellons condition. These issues were introduced in a Carnicom Institute webinar presented last year and the access to it is repeated here for your listening and review:
Listen to an Institute Research Discussion on Amino-Acids – Collagen
| The research interest, as a result of all of the above, now includes amino acids and proteins in general. If there is strong evidence to show that a host of amino acids are either diverted or disrupted to support the growth of the filament structure then there is an equally strong case to consider supporting the body with those same amino acids. Amino acids and proteins are structural features of the body that give it both form and function; these proteins are to be rebuilt if they are lacking in the body. There should be no hesitation in promoting the use of foodstuffs in the body and the proteins are once such main group. There are numerous methods by which one might accomplish such an increase, such as in the use of supplements, protein powders, diet and the like. No specific recommendations on that approach will be given here, but such means are readily available for all to consider. We have already considered whey (a particular protein form that has value with iron chelation). Gelatin is another form of protein that is strongly associated with collagen production. Protein rich foods and/or protein powders may be additional forms of nourishment that can be considered in light of the findings. Again, the reader has the responsibility to develop any health related strategies with the counsel of their own health practitioner and the information here is provided from a research standpoint only. |
Let us turn now to the issues of oxidation, oxidative stress and free radical damage. Our first clue that a serious issue with oxidation exists is with the repeated and definitive detection of highly oxidized iron within the biological filaments and the cultures that have been developed from them. Iron in the blood is required to be in the Fe+2 (ferrous) state to bind to oxygen; if the iron is changed to the Fe+3 state (ferric) it will no longer bind to oxygen and the primary function of the blood to transport oxygen transport throughout the body is no longer properly fulfilled. The iron in the biological filament is in the Fe+3 state; this means that an electron has been stolen from the iron in the blood in the Fe+2 state, and this represents a transfer in energy, in essence, from the blood of the human to support the growth of the organism.
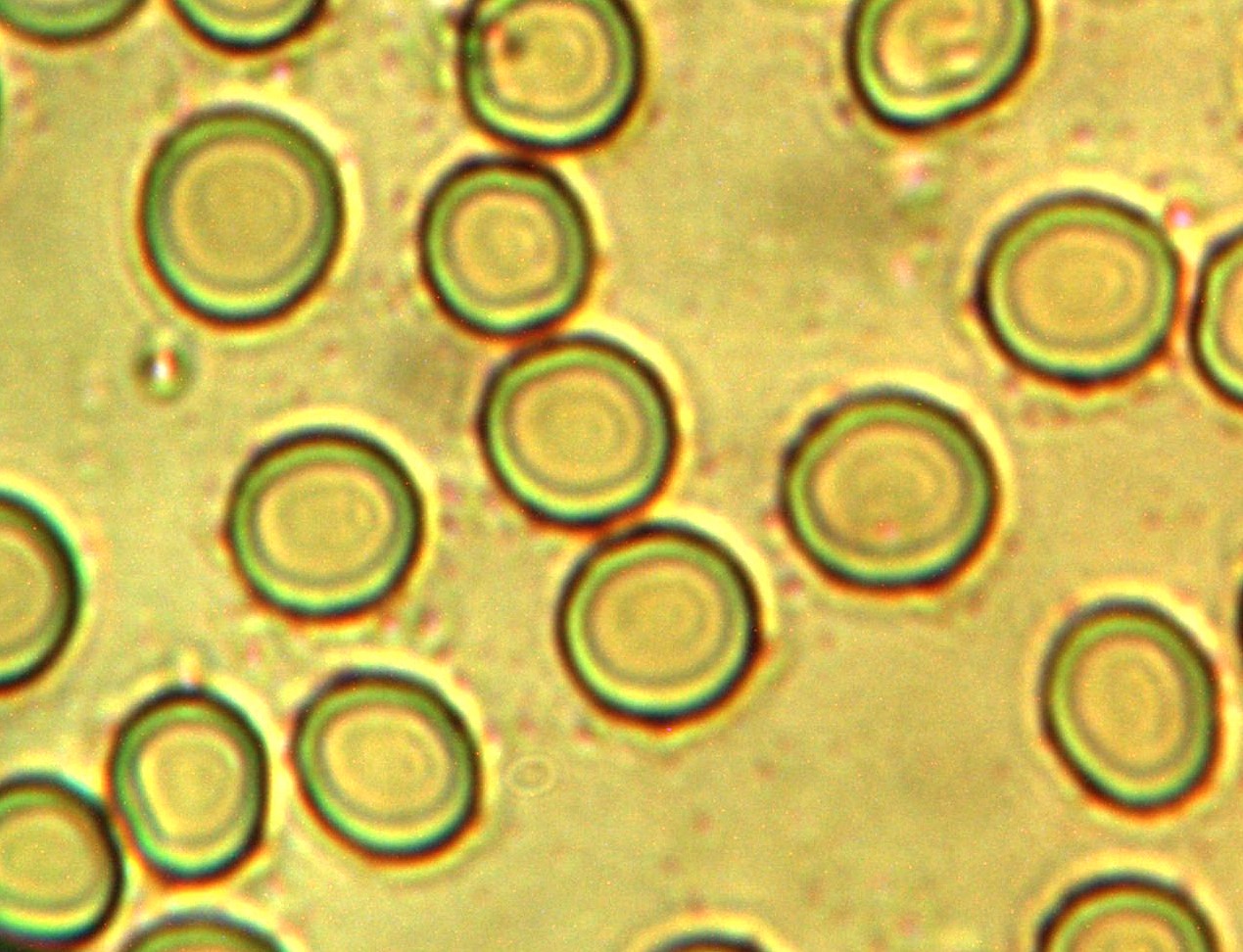
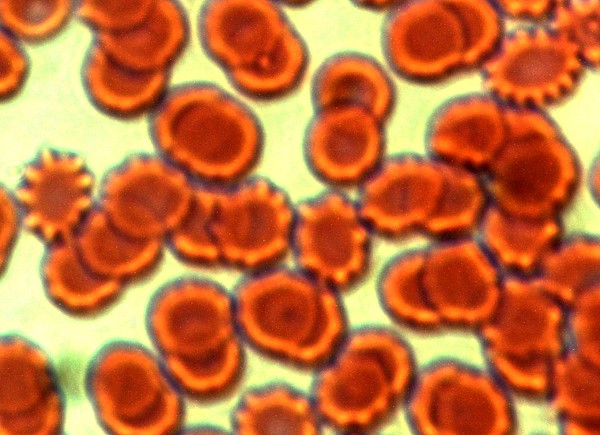
Another more direct method to investigate the state of oxygen carrying capacity in the body is to look at the blood under sufficient magnification. It has long been reported on this site that the integrity of the blood cells and the presence of the chlamydia-like bacterial structures within the blood are direct windows into the health impacts from the Morgellons condition. Please refer to the earlier paper (amongst others) entitled “A Mechanism of Blood Damage”, authored in December of 200969. In the table below are two blood slides of the same individual over a period of several years. The image to the left is during the earlier investigations of the blood as they relate to the Morgellons condition and as they were extensively reported upon within this site. The image to the right is of this same individual in a more contemporary state after considerations of the research within this site have been applied. Knowledge of the benefits of anti-oxidation strategies, along with the strategies to eliminate free radicals within the body, can potentially be demonstrated with these images as examples.
|
|
|
|
|
Examples of variability in general red blood cell integrity and the penetration of the cell membrane by the chlamydia-like organism within the blood. The oxygen carrying capacity of the blood is severely impacted by this breakdown in cellular integrity. The role of anti-oxidants and free-radical scavengers may be worthy of consideration in the improvements that are demonstrated in the image to the right. These images are of the same individual over a period of several years of research. It is of interest that the chlamydia-like structures appear to remain in the serum external to the cells in the image to the right; they do not appear, however, to be successful in breaching the cell membrane as they do in the image to the left. It is presumed that the state of the immune system is a primary factor in the defensive effectiveness. |
||

It is also of passing interest that a recently acquired commercially prepared human blood slide also shows this same detrimental blood condition upon sufficient magnification:
|
|
|
A commercially prepared human blood slide presumably representative of the general population. |
|
Some may consider this particular human blood slide condition as a coincidence or as irrelevant; others may be aware of strong claims by this researcher over the years that the general population appears to be subject (by varying degrees) to the health impacts of the “Morgellons” condition. Any recent statements by the National Institutes of Health (NIH) that classify “Morgellons” as a “rare condition” are in conflict with the assessment that has evolved from the research here. |
Another indication of excessive oxidative stress in association with the Morgellons condition derives from a study briefly mentioned within the earlier research report, “Morgellons : A Thesis”70. The particular section of the paper being referred to is entitled “A Proposed Spectral Project”. In this study, albeit with a limited sample, the results strongly indicate a deficiency in oxygen carrying capacity of the blood of a set of individuals claimed to be severely impacted by the Morgellons condition.
In addition, there is a body of anonymous functional medicine survey data made available to me that indicates severe oxidative stress conditions that are highly statistically significant within a separate set of individuals that claim to be severely affected by the Morgellons condition
Further, the functional group analysis from this paper reveals a host of structural features (identified, implied and plausible) that form a reasonable basis for the development of significant oxidative stress. These include (in addition to the oxidized iron – chlamydia-like presence situation), amino acid deficiencies, any cysteine deficiency, the presence of aromatic amines (with special attention to aniline or aniline-like structures, halogenated aromatic-amines and thyroid inhibitors in general, carboxylic acids and phenols (acidosis) and alkyl halides.
| If we assess that oxidative stress is likely a reality rather than a suspicion or conjecture, we then seek to address the problem with various strategies. Let us review what these strategies might include.
The first and most obvious consideration is the liberal use of anti-oxidants to combat an oxidative stress situation. First, we review what has already been presented once again in an earlier paper71:
|
I will further discuss and present resources on the topics of oxidative stress (from a health perspective) as well as “free radicals” in more detail to further emphasize their importance. As mentioned, oxidation is defined as the loss of electrons and reduction is defined as a gain in electrons. The process of exchanging, transferring or sharing of electrons has already been described as being fundamental to essentially all biochemical reactions; electron transfer is at the core of biochemistry. It is essentially the flow of energy within living organisms. An introduction to the importance of the oxidation stress and free radical issues as they relate to health is given as follows:
|
“Mounting scientific evidence may support the important role of free radicals in the development of some diseases. Free radicals are molecules or atoms that have at least one unpaired electron which usually increases the chemical reactivity of the molecule. Environmental radiation and physiological processes in the body cause free radicals to form. Free radicals can react with other molecules to cause cell damage or DNA mutation. Molecules called antioxidants protect against free radical damage. When antioxidants are ineffective, enzymes produced by the body work to repair free radical damage. Higher levels of free radicals tend to cause increased cellular damage. This effect is called oxidative stress. Oxidative stress may contribute to cardiovascular disease and cancer. Chemical compounds found in some foods may decrease the accumulated effects of oxidative stress, thus helping to prevent disease.75” |
As an alternative, the pathological approach of description to the relevance of oxidative stress and free radicals to health is as follows:
|
“One important mechanism of membrane damage…is injury introduced by free radicals, particularly by activated oxygen species. It is emerging as a final common pathway of cell injury in such varied processes as chemical and radiation energy, oxygen and other gaseous toxicity, cellular aging, microbial killing by phagocytic cells, inflammatory damage, …and others… Free radicals are chemical species that have a single unpaired electron in an outer orbital… the radical is extremely reactive and unstable and enters into reactions with ..proteins, lipids, carbohydrates.. and nucleic acids…Free radicals may initiated by oxidative reactions that occur during normal metabolic processes… Iron is particularly important in toxic oxygen injury… The main effects of these reactive species are on membrane, lipid bonds… of proteins and nucleotides of DNA76“ |
Another serious consequence of oxidative stress, and one that is increasingly important within the context of this paper, is that of neural degeneration. From the following paper on the subject of oxidative stress and neurodegenerative diseases77, we find that:
|
“Though, oxygen is imperative for life, imbalanced metabolism and excess reactive oxygen species (ROS) generation end into a range of disorders such as Alzheimer’s disease, Parkinson’s disease, aging and many other neural disorders….Antioxidants have a wide scope to sequester metal ions involved in neuronal plaque formation to prevent oxidative stress. In addition, antioxidant therapy is vital in scavenging free radicals and ROS preventing neuronal degeneration in post-oxidative stress scenario.” |
It is clear that the combination of any neurotoxin with that of oxidative stress, both of which are serious contenders in the research course underway, represents a serious threat to neurological health and functioning. The list of reported, observed and research-based health impacts of the Morgellons conditions must always be at the forefront in the setting of priorities for research. The evidence of neurological dysfunction in association with the condition deserves this spotlight in combination with the findings of this report. It is of no small interest that the commonly (i.e., formerly so) attached “diagnosis” of “delusional parasitosis” (even by supposed medical professionals) appeared at the onset of public knowledge of the condition and that this occurred prior to any proper investigation or research. It is fair to ask what motives and what knowledge base were in place to support such an a priori analysis and conclusion.
Continuing to present a series of references that further illustrates the extent of discussion with respect to oxidative stress, the following more comprehensive paper from Enrique Cadenas is also available78. In this paper, we find further clarification on what the term oxidative stress actually means. Metabolism, oxidation, and free radicals are an intrinsic part of the living process, and by themselves are not inherently “bad” or “good”. Cadenas explains quite simply that an imbalance between oxidants and anti-oxidants is what defines oxidative stress. This imbalance and “consequent damage to cell molecules constitutes the basic tenet of several pathophysiological states, including neurodegeneration, cancer, mutagenesis, cardiovascular diseases, and aging. A summary of free-radical formation, reactions, impacts upon health and various defenses against these effects is further detailed within this report.
A parting comment from referenced sources regarding oxidative stress is in order, especially as it relates to the iron situation. From the Alcohol, Research and Health Journal79, Wu Defeng, PhD discusses the role of metals in oxidative stress. He states that:
|
“Because of iron’s critical contribution to hydroxyl radical formation, anything that increases the levels of free iron in the cells promotes ROS [Reactive Oxygen Species] and oxidative stress” |
Recalling that free iron in the body is usually in the Fe+3 state (ferric) and that this form of iron is being definitively identified within the biological filament samples, it would seem as though the conditions for setting up an imbalance between oxidation and reduction (i.e., oxidative stress) have been satisfied.
It is also recommended that an earlier paper presented be reviewed at this time, entitled “Morgellons : A Discovery and a Proposal”80. In this paper a series of direct observations and trials that show interactions between biological filament cultures, iron in different oxidation states, oxidants, antioxidants and culture growth is presented. The results of those trials and observations are in complete accord with the expected biochemical reactions of oxidative stress that are being discussed here.
Now that information about the mechanisms of oxidative stress are amply available, It is time to start recalling the defensive part of the equation and to reiterate some of the many notable antioxidants that exist. These anti-oxidants form the basis for one of the primary mitigating strategies under consideration to reduce oxidative stress. Once we know the source of a problem and its likely impacts, we are in a much better position to make headway in solving it. This will be the case in terms of oxidative stress, and for other problems as well.
|
Returning to Robbins81 where the question was posed most directly, “Once free radicals are formed, how does the body get rid of them?” and he answers equally succinctly, with one very important addition in this round of the research: “There are several systems that contribute to termination of inactivation of free radical reactions. These include: 1. ..Antioxidants [e.g., vitamins, glutathione, cysteine, transferrin] 2. ..Enzymes [superoxide dismutase, catalase] 3. ..Glutathione peroxidase” [which catalyzes reduced glutathione] A definite pathway for research and consultation with health professionals has been charted here for anyone that cares to regard this information. I would encourage you to consider it and evaluate it accordingly. |
Let’s provide a specific example of what the oxidation process entails, along with important definition of what an oxidant is. An oxidant is known by several different names, all of which are the same thing, including, oxidizing agent, oxidant, free radical, or oxidizer. An oxidant, or free radical, by definition, is “any species that contains one or more unpaired electrons occupying an atomic or molecular orbital by itself.82” An oxidizer will essentially aggressively seek an electron from another species to form a bond with another atom or structure.
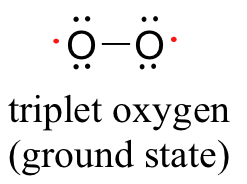
It is insightful to start the study by looking at oxygen itself, a major source of oxidation in its own right. The bonding between oxygen atoms is a fascinating case that defies conventional interpretations, and further examination will show that oxygen itself is a radical with two unpaired electrons, and it is therefore known as a diradical. This explains some of the reactivity characteristics of oxygen as we observe it, along with the interesting properties of paramagnetism (as can be shown with liquid oxygen experiments). Oxygen in the free state that we breath (O2) has the following Lewis structure83, 84, 85, 86:
|
|
| The diradical nature of oxygen, showing the two lone electrons of oxygen. The special reactivity of oxygen can be understood more readily with this interpretation and understanding of oxygen bonding. |
We are now in a better position to understand the sequence of free radical formation from oxygen as it forms within the body. In healthy cellular metabolism, roughly 98% of oxygen is converted to water with the remaining 2% involving free radical production87, and Cadenas shows us a sequential pathway that can take place, with the appearance of intermediate free radicals along the way ( superoxide anion and they hydroxyl radical)88:
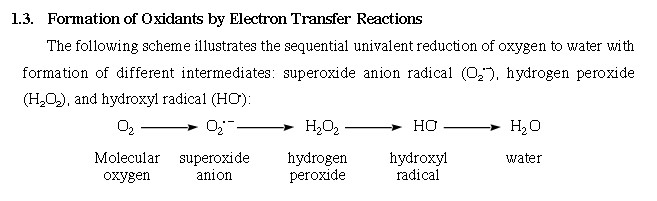
Source : Enrique Cadenas, PhD
In more common language, we have the following description of the situation89:
|
“..oxidants or free radicals are the major cause of over a hundred human diseases. The process of ageing is also hastened by the onslaught of oxidants in the body. Oxidants are normally produced during healthy cellular metabolism, wherein 98 per cent of the oxygen consumed by a cell is converted to water. The remaining one to two per cent of the unutilised oxygen is free to escape as free radicals. Free radicals or oxidants are molecules containing single unpaired electrons, and are on the lookout for electrons to pair up. Examples of oxidants are superoxide anion, hydroxy one radical, reactive oxygen species like peroxides, hydroxides and singlet oxygen.” |
The emphasis upon oxidative stress being an imbalance in the equation above is described again here, again in more generalized terms90:
|
“When the body’s antioxidative defences are inadequate, or when the supply of nutritional antioxidants is unreliable, or when the oxidant attacks are consistently alarming, the state of balance is tilted from a state of health to a state of slow degeneration.” |
With this increased understanding of the route of oxidation within the body, let us return to the topic of countermeasures to oxidative stress. Fortunately, understanding the nature of the problem does place in a stronger position to pursue countermeasures. The recurring theme of the role of antioxidants is quite evident in the literature and health related papers available to us all; we simply must avail ourselves to them. Again, methods of mitigation are clearly portrayed in the Pharmaceutical Field article:91
|
“Over the years of evolution the human body has developed a whole arsenal of antioxidative enzyme systems and vitamins for its protection. Antioxidant systems of the body are critically dependent upon external dietary sources. What are these exogenous antioxidants and where are they found? Natural Antioxidants To The Rescue Vitamin A and its polymers are available from brightly coloured vegetables and fruits such as carrots, apricots, dark green leafy vegetables like spinach, red, yellow and green peppers, sweet potatoes, and blue-green algae. Vitamin C is obtained from lemons, limes and other citrus and sour fruits. Vitamin E is found in nuts, whole grains, vegetable oils and to some extent in fruits and vegetables. In general, minerals are available naturally from fruits, nuts and lentils, whole cooked and germinating grains, shell-fish, vegetables and many others. Many other naturally occurring antioxidants that have been studied are pycnogenol from pine bark, grape seeds and red wine, lycopenes from tomatoes and beets, and coenzyme Q10 from red lean meat and blue-green algae. Garlic, tea and blueberries are also rich in natural antioxidants. Conclusion |
We continue to consolidate and extend our arsenal against oxidative stress, this time with a short presentation from the University of Colorado. In the paper entitled “Free Radicals and Reactive Oxygen”, we find a helpful section at the tail of the article. Two different classes of antioxidants are presented in this approach, those that are enzymatic in nature and those that are non-enzymatic. More explicitly, the section of interest is as follows:
|
“Mechanisms for Protection Against Radicals Life on Earth evolved in the presence of oxygen, and necessarily adapted by evolution of a large battery of antioxidant systems. Some of these antioxidant molecules are present in all life forms examined, from bacteria to mammals, indicating their appearance early in the history of life. Many antioxidants work by transiently becoming radicals themselves. These molecules are usually part of a larger network of cooperating antioxidants that end up regenerating the original antioxidant. For example, vitamin E becomes a radical, but is regenerated through the activity of the antioxidants vitamin C and glutathione. Enzymatic Antioxidants Three groups of enzymes play significant roles in protecting cells from oxidant stress:
In addition to these enzymes, glutathione transferase, ceruloplasmin, hemoxygenase and possibly several other enzymes may participate in enzymatic control of oxygen radicals and their products. Non-enzymatic Antioxidants Three non-enzymatic antioxidants of particular importance are:
In addition to these “big three”, there are numerous small molecules that function as antioxidants. Examples include bilrubin, uric acid, flavonoids and carotenoids. |

Readers may notice the level of overlap and correspondence that is now becoming evident in the specific compounds and substances that are regarded as highly effective antioxidants. One may refer to the previous section from the pathology textbook that emphasized the role of antioxidants, superoxide dismutase (SOD), catalase and glutathione peroxidase to become aware of certain standards that have evolved in the oxidative stress research. The special emphasis upon glutathione should also be noted, to the effect that93:
|
“Glutathione may well be the most important cellular defense against damage by reactive oxygen species [free radicals]“. |
Continuing the discussion on the importance of glutathione as an antioxidant, it is highly relevant to again recall the previous research paper entitled, “Morgellons : The Breaking of Bonds and the Reduction of Iron” from November of 201294. This paper chronicles in depth research that describes the important role that glutathione is anticipated to assume in the mitigation of the Morgellons condition. There are strong conclusions arrived at within this report, particularly those that concern the ability of glutathione to break down bonds in the identified proteinaceous structures, as well as the ability of glutathione to reduce the oxidation state of iron. It is thought that it may be highly beneficial to review the research presented in that earlier paper, as the proposals mentioned are now only further corroborated with the current research. The link to this paper is presented immediately below:
Morgellons : The Breaking of Bonds and the Reduction of Iron
It may also be worthwhile to become familiar with an independent physician’s evaluations of the Morgellons issue and to take note of the acknowledgement of the prospects for glutathione benefits within that same paper95:
Morgellon’s : The Role of Atmospheric Aerosolized Biological Nano-Particulates
A few other points related to the glutathione issue bear repetition within this current collection. It has been described in earlier papers that glutathione is another one of the cases where direct supplementation may be of little value. If we suppose that a body is lacking in a particular compound, substance, or enzyme, for example, a common instinctive reaction by many is that somehow it should simply be taken as a “supplement” to fulfill that deficiency. This approach can be both unwise and foolhardy as our previous discussion on iron substantiates. When information becomes available, it is of little value unless it has been interpreted properly and comprehensively. It is another of the many reasons that professional health and medical counsel is to be sought and why education must be a lifelong pursuit. There are risks in assuming that we know more than we do. In that discussion, it was communicated that direct ingestion of glutathione appears to be of marginal value in human health. The emphasis in glutathione production within the body appears to revolve heavily around the precursor biochemistry of glutathione, more than with glutathione directly. The role of N-acetyl cysteine (NAC) has already been discussed in that regard in the previous papers mentioned. It may be wise to become familiar with that the role of “precursors”, especially as they relate to the glutathione issue. Over simplification of a problem and the seeking of immediate rewards without proper understanding and comprehension can have their own price in our lives. The case for immediate and intensive participation by the health and medical communities to solve the health problems before us is patent.
Another topic of developing interest, especially in light of the current research findings, is the role that glutathione may assume in combating neural disorders, such as Parkinson’s Disease. We are forced to consider the prospect of neural toxins (e.g., oxydopamine related compounds or structures) as being a potential component of the biological filament growth form. This discussion has already taken place within this paper to some extent. What is of interest here is to reacquaint ourselves with an introductory library of media on the glutathione issue, as also available in the earlier paper referenced96.
|
|
|
|
|
Dr. Mark Hyman |
Dr. Don Colbert |



(No endorsements of products or services to be implied or stated herein)
|
|
|


(It may be of benefit to research additional presentations by these and other speakers on the issues of
glutathione, oxidative stress, chronic diseases and neuro-degenerative conditions)
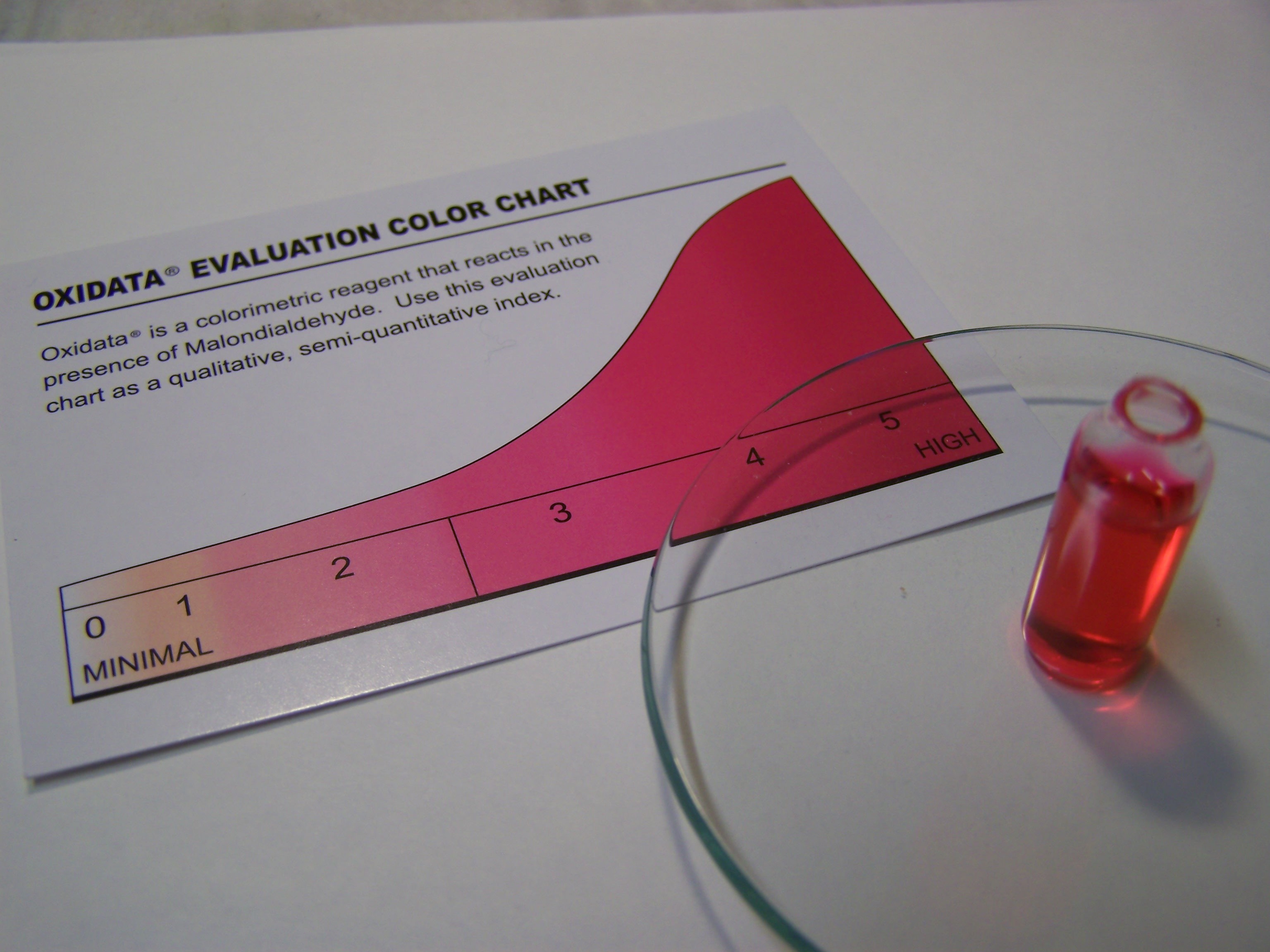
An accessible and relatively inexpensive test (~$20) is available to test for oxidative stress in the body; this appears to be a highly valuable piece of information to assess with respect to the impact of the Morgellons condition and health in general. A body of information at an anonymous level is available to this researcher and it does indicate that oxidative stress may be an especially important factor, as the research also shows in numerous and substantial ways. The details of this colorimetric test are available at the manufacturer’s site96b and it may be found through numerous sources available to the public96c. An example of a urine test result for one individual is shown below:
|
||||||

The following topic is deserving of more consideration in the future, but the relationships between antioxidiants, minerals and enzymes has been made more than once along this journey of discovery. As one pharmacist relates (now from a perspective which emphasizes nutrition), speaking of reactions that involve antioxidants96d:
| “Most of these reactions need something called an enzyme to make them work. And many of these enzymes are actually antioxidants themselves- your body even makes them- that’s how important antioxidants are! Many minerals are vital parts of these reactions too, even though they’re not antioxidants themselves (so they’re equally important to have). These include selenium, manganese, copper and zinc.” |
Clearly, there is more research and work to do, but the point has been made, and I suspect that it is an important one.
The next impact upon health that we transition to is that of excessive acidity, or acidosis. There is significant evidence from the research of record to implicate a serious acidic component to the Morgellons condition. The effects of excessive acidity in the body have been previously discussed, including demineralization, low energy, dental decay, weak immune system, chronic digestive problems, joint pains, bacterial and fungal infections, and many others. Please review that section of this paper to recall the numerous and significant health effects that can accrue from over-acidity within the body. Our desire here is to suggest what means might exist to counter the many problems are know the result from acidosis, and to suggest means by which extent of the problems might be monitored.
Researching the available literature, it is apparent that there is a fair amount of controversy regarding the strategies to counter the effects of excessive acidity. There are individuals that claim that eating certain food groups are effective at changing the acid state. There are individuals that claim that drinking water that is alkalized, often by various devices or with additives to the water, will result in beneficial effects. There are individuals that claim that testing the pH of either urine or saliva is representative of the body chemistry. There are individuals that will attempt to refute all of the above claims. This section of the paper is neither to advocate or to dismiss potential methods that be beneficial; it is to increase awareness of the importance of the issue and to provide a modicum of education to point the reader to various possibilities for further research, advice or action. The process of becoming aware of an idea or method does not imply or state endorsement, agreement or disagreement for that matter; it is to inform us of choices and research ideas. What is clear is that a fair amount of controversy exists on this particular subject; usually in such cases there is an abundance of misinformation or disinformation (intentional or otherwise) that must be sorted through. The profit motive of advocating certain and particular strategies, means, products and devices must also be considered in this regard.
One method to approach this problem is to focus, at an introductory level, on the medical condition of acidosis and to learn what are the identifying characteristics of that problem. The term itself is usually used in a strict medical sense applying to reduced pH of the blood, however, it is also sometimes used to express generalized excess acidity at the cellular and tissue level. Acidosis in the strictest sense of the term may well be a medical emergency, but we can use a study of that condition to our advantage to understand what systems of the body are being most seriously impacted. It may then be considered from that point on as a matter of degree as to how much the body may be impacted by excess acidity and to what extent.
We can start with the definition of acidosis itself. Acidosis is an “increased acidity in the blood and other body tissue. If not further qualified, it usually refers to acidity of the blood plasma”97. Note here that there is no requirement from the onset to restrict our discussion to the issue of blood only, as it is not required by definition. The measurement of blood acidity (pH) is not a common affair for the majority of us, and we prefer to not restrict our methods of measurement to that method alone. Another very important statement within this same article to recognize is that “the rate of cellular metabolic activity affects and, at the same time, is affected by pH of the body fluids”98. We will keep this statement close at hand, as we shall see that the issue of cellular metabolism will be at the heart of excess acidity within the body.
We can once again see that we are in no way restricted to the consideration of blood alone when we are dealing with the determination of acidity within the body. Measurement of additional body fluids, such as saliva and urine, already appear to be reasonable to consider in our scope of acidity assessment, especially in a relative sense. It is also a fact that the pH of urine is regularly used as a diagnostic aid in the medical professions. Low pH values (i.e., high acid) of urine are indeed indicative of acidic conditions within the body, especially for those at risk of producing urinary stones99. The measurement of the pH of urine does indeed appear to be a viable point of measurement for acidic conditions within the body. One might also presume that such measurements could also be useful in a relative sense, i.e., to indicate changes of acidity within the body over a period of time.
Before seeking out the root causes of acidosis, it is worthwhile to mention that acidosis comes in two primary forms, metabolic acidosis and respiratory acidosis. Metabolic acidosis can result from the increased production of metabolic acids (please recall the discussion of organic acids earlier in this paper and the relationship to the carboxylic acid functional group) and kidney disturbances that excrete excess acids. Lactic acidosis is a form of metabolic acidosis and it is characterized by low pH in the body tissues and blood. Respiratory acidosis results from a buildup of carbon dioxide in the blood.
An investigation into the research literature reveals two strong recurring themes as the basis and cause for acidosis. The first of these will center on the issue of incomplete metabolism under conditions of reduced oxygen and the second will involve the depletion of minerals. We will now begin to document these important threads which immediately tie in with the leading statement that we called attention to:
| “the rate of cellular metabolic activity affects and, at the same time, is affected by pH of the body fluids“ |
We refer to Dr. Michael Lam, once again, for a more lay interpretation of the importance of pH to body chemistry and for important sources of acid increase within the body. Dr. Lam will also reveal to us the primary mechanisms by which the body compensates for this change. Furthermore, Dr. Lam will make the case in his article100 that diet, in addition to other measures, is indeed a significant factor in affecting a change in acidity within the body. This will come as no surprise as we investigate further the root causes of acidosis.
| “One of the key determinants of the speed of aging and onset of degenerative diseases is the internal biochemistry and terrain of the body. Internal biochemistry is best measured and discussed in terms of the pH.”
“The term acidosis is relative and only meant to convey a shift in total body chemistry towards the acidic direction.” The principal sources of acid buildup are: 1.) The metabolism and/or incomplete breakdown (oxidation) of foodstuffs or metabolic “waste” produced as a by-product of cellular activity. During normal cellular respiration and energy production , acids as produced as part or “waste” products. These acid must be “balanced”, neutralized, or removed by the body’s buffering and detoxification systems through the kidneys, lungs, liver, and blood. 2.) The consumption of acid present in the food, air, and water supply. Nitrogen emissions from automobiles and industrial plants, food dyes, sprays, waxes, preservatives, additives, artificial sweeteners, fertilizers, water pollutants, and even chloride and fluoride in tap water are just some of the highly acidic chemicals are ingested by millions everyday. How does the body overcome the acidity? The body undergoes an natural and ongoing balancing act constantly. Underlying regulatory forces work continually to balance an acidic body chemistry to remove excess acid and return the body to a more neutral state. These internal buffering mechanisms include: a. The production of bicarbonate from the organs and cells of the body. b. The removal of minerals such as calcium from bones to be used as buffering agent to neutralize the acid. This is one of the leading causes of osteoporosis. c. The blowing off CO2 or carbon dioxide from the lungs. Carbon dioxide is an acid. It leads to symptoms of shallow breathing and hyperventilation. d. The release of alkaline bile from the liver and alkaline digestive secretions from the pancreas and the retention of sodium from the kidneys in response to the secretion of the hormone Aldosterone. Aldosterone is produced from adrenal gland, and stimulation of this gland leads to the feeling of internal “stress”. |
For those seeking a somewhat more detailed explanation of how the body compensates for an imbalance in pH, it is instructive to examine the medical model approach. In the paper entitled “Acid Base Balance in Critical Care Medicine101“, we find a modeling process that is applied to this problem that further confirms the statements in lay language by Dr. Lam above. This model introduces the balance that occurs in the body extracellular fluid between positive and negative ions, primarily that of sodium, potassium, calcium and magnesium on the positive side and the chloride ion on the negative side (i.e., Strong Ion Difference). Furthermore, it will be stated that a decrease in these positive ions will increase the hydrogen ion concentration (the very definition of an acid) through the buffering system in the body, resulting in acidosis.
This modeling process is essentially equivalent to what has been stated by Dr. Lam, i.e., demineralization will accompany acidity within the body.
Acid-base chemistry in the body can become a complex affair, and a detailed examination of the situation, factors and chemistry can be found at Dr. Grogono’s site entitled “Acid-Base Tutorial102“. A good introduction to acid-base chemistry is provided at the onset, where the two essential factors are described as follows:
| “The Bird’s Eye-View, Two Components:
Respiratory: When breathing is inadequate carbon dioxide (respiratory acid) accumulates. The extra CO2 molecules combine with water to form carbonic acid which contributes to an acid pH. The treatment, if all else fails, is to lower the PCO2 by breathing for the patient using a ventilator. Metabolic: When normal metabolism is impaired – acid forms, e.g., poor blood supply stops oxidative metabolism and lactic acid forms. This acid is not respiratory so, by definition, it is “metabolic acid.” If severe, the patient may be in shock and require treatment, possibly by neutralizing this excess acid with bicarbonate, possibly by allowing time for excretion/metabolism.” |
| As we continue to strike toward the heart of acidosis, at least from the more critical medical emergency perspective, one cannot help but notice that efficient aerobic respiration, complete metabolism and the lack of oxidative stress are at the absolute core of the issue. These issues have emerged time and time again within this current research, and it would be foolhardy to ignore this deep-seated theme at this point. In addition, we have learned that demineralization of the body (e.g., degradation of bone and teeth as examples) are expected to occur as a result of an acidic condition because of the body’s natural buffering systems that attempt to maintain ionic balance within the blood and body fluids. |
The topic of excess acidity was first posited several years ago, in the paper (2010) entitled, Morgellons : A Discovery and a Proposal103, where attention was called to the following:
| “In the culture environment, it has been established that the organism(s) flourish within an acidic environment. In addition, it has also been stated in earlier reports that many biochemical reactions only take place within a narrow pH [acid or alkaline] range. Therefore, one of the first strategies to consider is to change the acidity or alkalinity of the growth environment and see if progress results. What has been observed in the cultures thus far is that an increase to the alkaline side does indeed appear to inhibit the growth of the culture.” |
In a succeeding paper (2010) we find the following conclusions that were presented104:
| “The growth of the bacterial-like organisms that appear to be at the foundation of the so-called Morgellons condition has been positively inhibited…The basic strategy that has been adopted is a transformation of the growth environment to a more alkaline condition along with adding specific antioxidants that are directed toward the scavenging of the hydroxyl radical. |
We turn now to an additional important means to alkalize the body, that of bile production by the liver.
Attention was called in 2011 to the role of bile as one of several mitigation strategies listed in the paper, Morgellons : A Thesis105(2011):
| …”Improving the flow of bile in the system to further alkalize the body and aid the digestive system. The liver, the gall bladder and the bile duct play an extremely important role in alkalizing the digestive tract. For those that demonstrate a persistent acidic condition within the body it may be beneficial to learn of the importance of bile production and its alkalizing function.
An acidic condition can easily be created with a blockage of the bile duct, as the bile is the alkalizing agent within the intestine. Gall bladder removal and gall stones appear to be a frequent occurrence; this would suggest that overloads of toxicity to the liver could well be at the root of this problem. Non-invasive methods of breaking down gall stones (conglomeration of bile) are available to consider, such as Chanca Piedra (breakstone). If the bile flow is restricted, an acidic condition within the body is expected to exist. Knowledge of the physiology of the liver, gall bladder, bile duct and its relationship to digestion may be beneficial in mitigating the consequences of acidity within the body and digestive system.” |
| Furthermore, the reader was introduced at that same time to an educational video on the relationships between the liver, bile production, acidity, alkalinity and immunity was made available at the following site:
Video Series: Liver, Gall Bladder and Bile Duct Physiology (No endorsements of products or services to be implied or stated herein) |
There are recent observations of liver tissue that are important to be briefly introduced at this time; the subject will be discussed in more detail at a later date. If the body is unable to process the toxic load placed upon the digestive system, there will be an accumulation of these toxins within the body. The function of the liver is manifold, and detoxification and waste removal is foremost on that list. The liver is also responsible for protein synthesis, the breakdown of fats with the production of bile, glycogen storage, decomposition of red blood cells, iron regulation, and many others. We only have one liver and we cannot afford to have a serious problem with it.
One of the major problems with the liver (of increasing incidence) is the accumulation of fatty tissue within the liver. It is estimated that more than 1/3 of the population now suffers from fatty liver disease that is unrelated to excess alcohol use. The net impact from the accumulation of these toxins is an enlarged and fatty liver. If the liver is unable to process the toxic overload, fat cells with the toxins will accumulate and be stored within the liver. It is potentially a serious situation and one that is difficult to reverse quickly; weight gain is often associated with the condition. What follows is a photographic comparison of a healthy and a fatty liver:
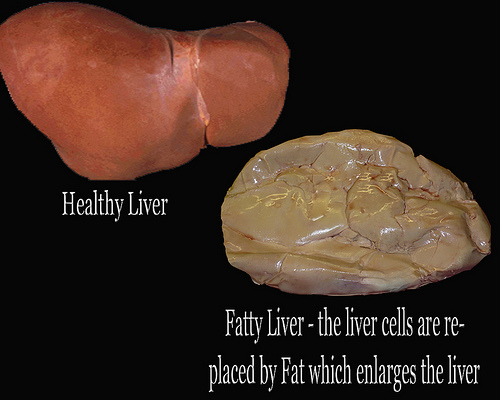
source : www.healthadvice4life.com
From visual impressions alone, it is clear that this condition is not a healthy one. It is reasonable to conclude that the functioning of the liver is seriously impaired with this condition. We can also find examples of what the fatty liver looks like under the microscope, also in comparison to healthy liver tissue:
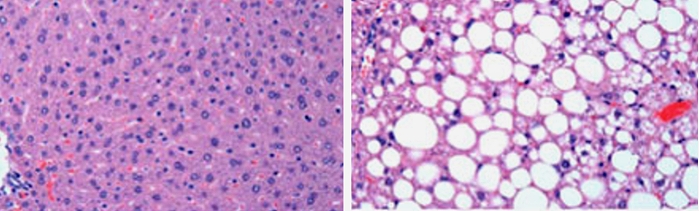
Comparison of normal liver tissue(left) and fatty liver tissue (right)
source : advance.uconn.edu
Recent observations of calf liver under the microscope show this condition of fatty issue existing. There are two concerns present from this initial observation:
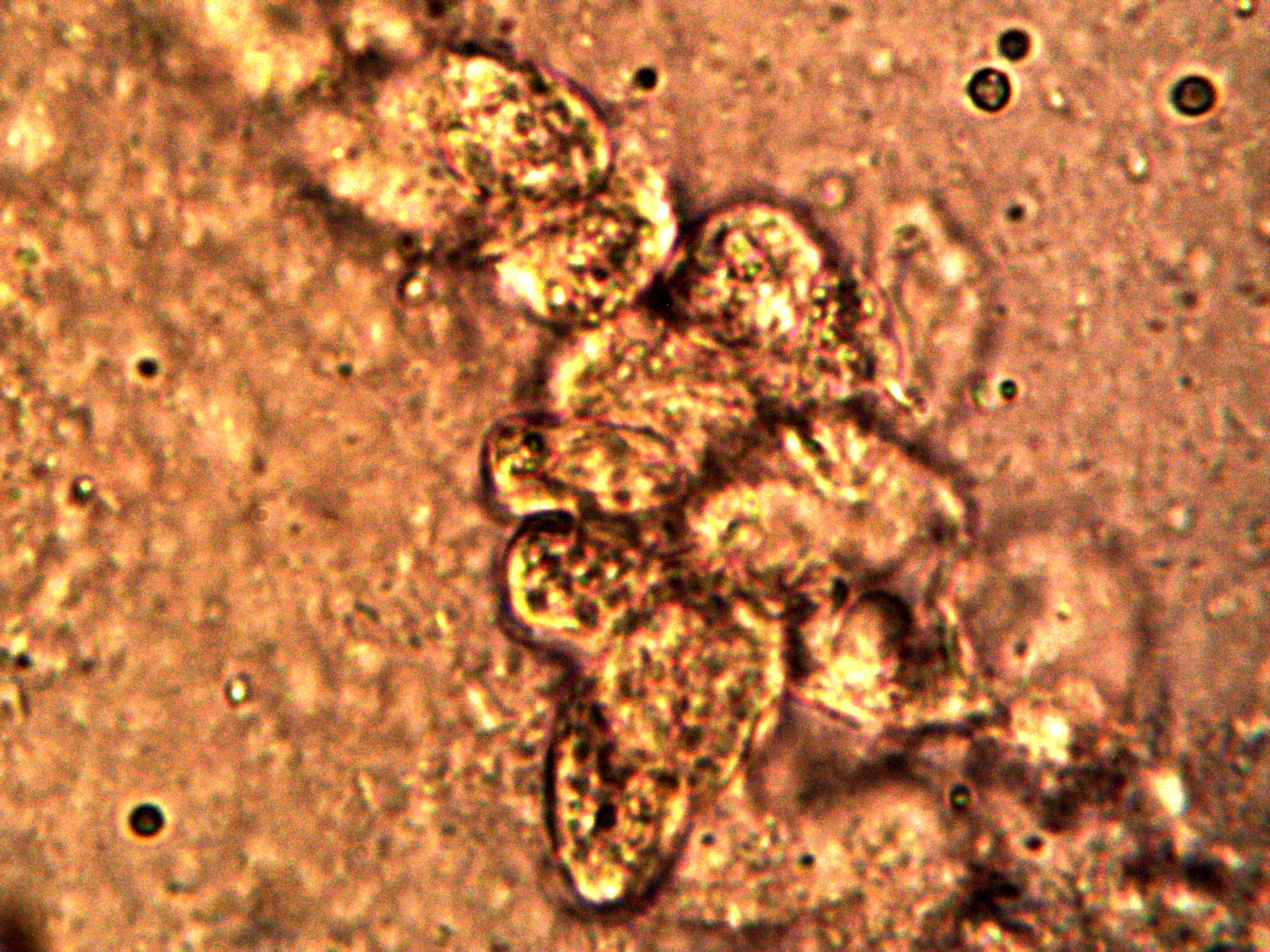
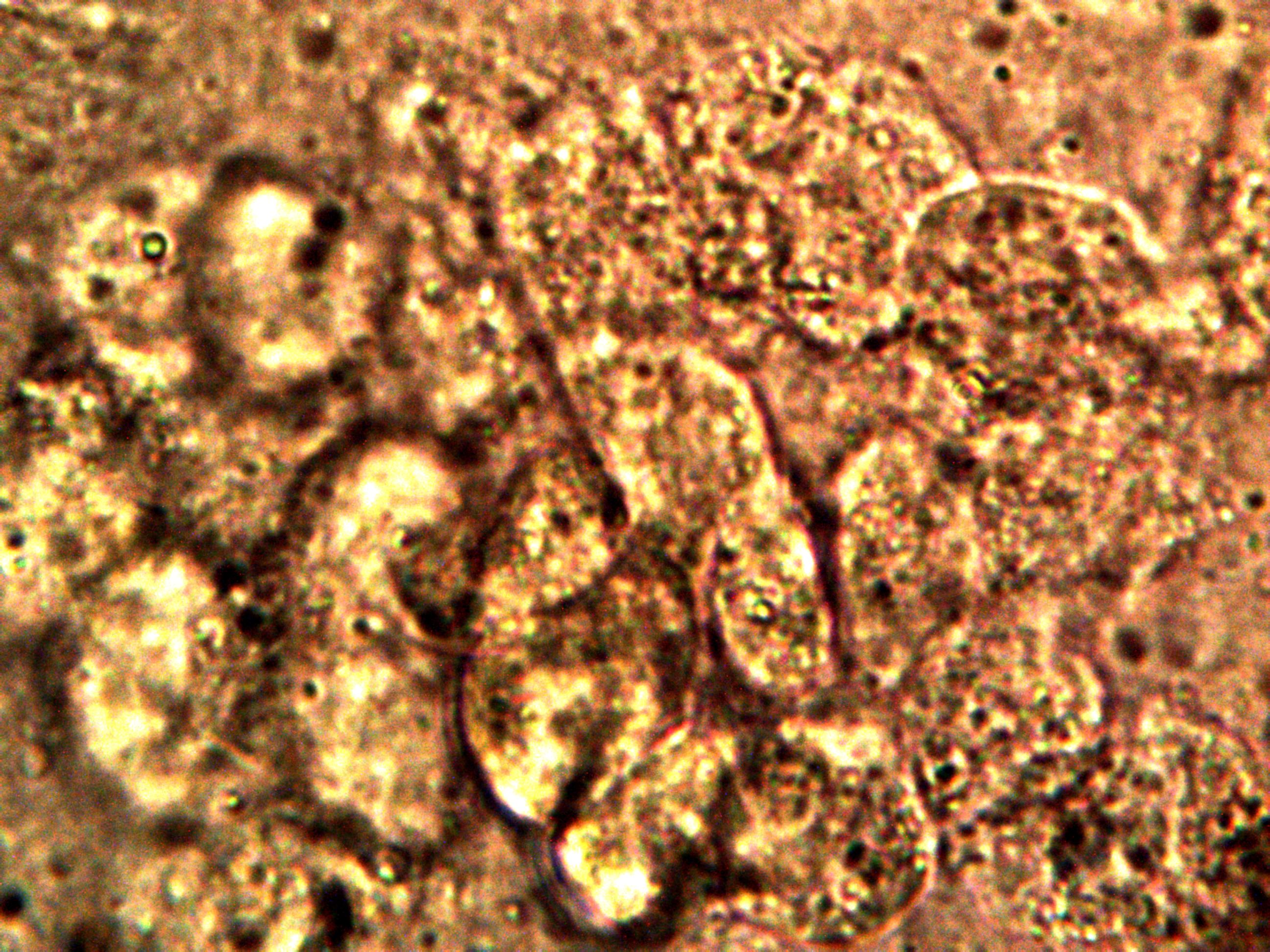
Appearance of significant fatty liver tissue within a calf liver recently analyzed.
Sub-micron bacterial-like structures (identical in size and shape to those studied extensively on this site)
are abundant within the fatty cells. Magnification approx. 8000x.
1. The animal is young, and therefore excess fatty tissue would not be anticipated at this stage of growth.
2. The fat cells are enclosing large numbers of what appear to match (identical in size and geometry) the sub-micron, bacterial-like structures that are the subject of much scrutiny within the research of this site and this current paper.
It is reasonable to surmise that the abundant presence of the encapsulating fat cells represents a toxic-overload response by the liver in the young animal. Other issues of equal and concern arise from this recent observation; this research is to be presented at a later date.
For numerous reasons, there is a legitimate case for concern about the impact of the Morgellons condition upon the functioning of the liver; this includes potential toxic overload, fatty tissue development and the prospect for an enlarged liver that results. If such proves to be the case, there is an obvious need for consideration of liver detoxification strategies to be incorporated within this report.
Although he have now forged through some of the controversies regarding acid-base imbalances, it is certain that some shall remain after this paper is complete. The issue of drinking water that has been “alkalized” must be given mention, however unappealing the circumstances may be to certain parties along with their particular knowledge base. There are those that advocate that certain alterations of water, either chemically or with certain devices and technologies, will be sufficient to address the acid-base imbalances under study here. I do not find such arguments, thus far, generally sufficient to justify such conclusions at this point. It is evident from the work at hand that sufficient oxygen available at the cellular level, thorough aerobic metabolism, reduction of excess carbon dioxide, mineral balance, diet (especially as it relates to mineral intake) and the alkalizing processes of the body (e.g., bile production and flow) are at helm of acid-base balances within body and health. The argument for a modification of the “water molecule” (under question in its own right) to account for and compensate for the complex systems mentioned above appears that it may be lacking in the necessary substance of this problem. Whether one “agrees” or not with the following information from Dr. Lawrence Wilson on the topic of “alkaline” water, it behooves us to become familiar with the arguments put forth106:
| “The pH balance of the body is very important, and most people’s bodies are too acidic at the cellular level. It does not matter if the saliva, urine or other fluids test alkaline. In almost all cases, the body cells, which is the site of metabolism, are too acidic. This predisposes one to many metabolic imbalances and diseases including cancer. The rationale for drinking alkaline water is that it will correct this important physiological imbalance.
Problems with this rationale for alkaline water. The main problems with this theory are 1. The real cause of excess acidity at the cellular level is a deficiency of what are called the alkalinizing or alkaline reserve minerals. These come from what one was born with, and from the diet. If one lives a stressful life, one also depletes these quickly. They include calcium, magnesium, zinc, selenium, and a few others. Unfortunately, drinking artificially alkalinized water does little or nothing to replace these vital minerals. In fact, it may deplete them for unusual reasons. It may make the body think it is alkaline, so the body does not need to hold on to its alkaline reserve minerals as much, and it eliminates some of them, making the person even more deficient. 2. Water from alkaline water machines replaces the vital minerals with a little cadmium, lead, arsenic and other toxic metals found in tap water and not filtered by any carbon filters that I am aware of. Some filtering systems claim to filter out toxic metals, but I have not observed this in practice. Those filters that I have seen that are said to remove a lot of toxic metals tend to damage the water even worse. Reverse osmosis is an example of this type, along with KDF and other types of “advanced” filtration media. 3. In addition, the alkaline water machines also replace the good minerals with a little platinum and titanium found in the plates that the water passes over to make it alkaline. These are both supremely toxic metals, especially platinum. In addition, I have observed slightly higher levels of nickel in those who use alkaline water machines for several years. The nickel is probably leached from the stainless steel in the machine, or perhaps from a nickel-plated machine part. Nickel is a deadly toxic metal. The alkalinity of the water may cause a little to be leached out of the machine parts. 4. Carbon filtration also does not remove enough of the toxic chemicals in the water, so one is also getting a dose of chlorine, fluorides, aluminum, copper, residues of medical drugs in many areas, pesticides and more. 5. As a result, alkaline water machines do not really balance the body’s pH, although they will change it a little, giving some people the impression they are getting well when, in fact, they are becoming more ill. The only way to truly balance the body is to replenish the alkaline reserve minerals. To do this, one must eat a lot of cooked vegetables. The cooked vegetables, and perhaps some mineral supplements, when carefully chosen such as kelp, can and do supply the alkaline reserve minerals. Good quality, natural spring water also supplies some alkaline minerals, as does good quality sea salt. Using these on a daily basis, the body can be slowly remineralized. This is the way to do it, not drinking artificially alkalinized water.” |
We can once again see the emphasis upon the alkaline reserve minerals as a major pathway toward the restoration of the acid-base imbalance, with an emphasis upon diet to accomplish this. The verdict on exotic or expensive technologies to alter the “state” of water is left to the reader to investigate further; I would only encourage that the study be rooted in chemistry, biochemistry and physics as opposed to promotional claims. At this point of study the causes of and factors affecting increased acidity, from numerous and varied sources, parallel the summary given by Dr. Lam to us at the onset (please review) remarkably well. These include incomplete metabolic breakdown of foods and nutrients, the lack of availability of sufficient alkaline reserves, the ingestion of acidic toxins or foodstuffs into the body, carbon dioxide imbalances and the failure of the bile system to adequately alkalize the intestinal tract. The road to recovery from the impact of such damage is to reverse the courses above, i.e., increase the efficiency of the oxidation of fuel, assure adequate oxygen in a form that the body can actually use, intake sufficient alkalizing minerals (such as calcium, magnesium, etc.) and improve the flow of bile and improve the digestive processes in general. It is obviously a tall order, but courses of action are readily available to all of us. Consultations with health practitioners about the sensibility or validity of the information being relayed here is a good start in the process. Supporting this process with your own studies and research on the matter can only be of further benefit.
For those that continue to profess that what you consume does not materially affect your body chemistry, or for that matter, the acid-alkaline imbalance in general, let us cite a more traditional example from the American Journal of Clinical Nutrition on the subject of diet, pH and oral health. It states clearly that what we eat is not a neutral affair107:
| “..Diet affects the integrity of the teeth; quantity, pH, and composition of the saliva, and plaque pH. Sugars and other fermentable carbohydrates..provide substrate for the actions of oral bacteria, which in turn lower plaque and salivary pH. The resultant action is the beginning of tooth demineralization.” |
Readers may once again be struck by the association between acidity and demineralization; the relationships between diet, body chemistry, acidity and alkalinity are all too apparent in the literature.
The preceding section serves as a welcome segue into the realm of what may be rather unsung heroes; those that have devoted themselves to health, nutrition and “functional medicine”. Many of us look to a particular type of “doctor” to “heal” an ailment or disease, but those that study the role of nutrition in promoting health and those that study health in a more holistic sense are likely our true and best allies. There are many individuals that have studied extensively the relationships between oxidative stress and acidity, for example, with nutrition and the body systems in an integrative sense. It is wise for us to avail ourselves of their talent and knowledge, as opposed to only seeking a particular “cure” to a “particular ailment”, including that of “Morgellons”.
If we now open our discussion to include the counsel of those that study nutrition as a lifelong passion and its role in our health, the association between health and the acid-alkaline balance is prominent within the literature. For those that continue to advocate that saliva and urine pH have no real value in the assessment process, it may be prudent to become familiar with a portion of the following discussion. For those that seek out the credentialing process, Dr. Biamonte is no lightweight in the profession of clinical nutrition. One article worth studying in detail is entitled, “Urine and Saliva pH Testing”108 from the Biamonte Center for Clinical Nutrition. A few excerpts are in order here, but it is advised to study the article in detail. The acid-base balance discussion, the role of minerals (once again) in the process, and various simple testing procedures for both saliva and urine are worthy of your consideration. Please conduct your own research with the critics as well and reach your own conclusions as to motives and intentions of various parties. You may also wish to examine the documented effects of demineralization and destruction of teeth and bone documented earlier in this paper, as well as to study those that have suffered from these effects. The mineral loss in these cases is clear and evident, and it is difficult to deny that the acid-base balance is an important part of the process.
In the meantime, let us proceed with some representative sections from the article:
Along the course of the article, Dr. Biamonte also introduces us to the “lemon-test”, a relatively simple test that can be used to give an indication of the available mineral reserves in the body. The history of the test and its use extends well beyond any single practitioner, and it is also described in some detail by Dr. Dicken Weatherby in his book on functional medicine, “In Office Lab Testing : Functional Terrain Analysis109“. Various examples of test results are described within this same book. The origin of the test appears to reside with a Dr. Henry G. Bieler, MD.110, the well known author of “Food is Your Best Medicine”.
|
|
|
The introduction to the pH Saliva test, from |
I have witnessed the administration of the test locally, and I find the results to be of much interest and expressive of variation between individuals. The test is simple enough in principle and practice to monitor individually if desired, as in the following example with two separate individuals.
|
|
|
|
| The Acid-Lemon Test conducted by two separate individuals. The individual on the right demonstrates a stronger decrease in pH over the time interval measured. The reasoning behind this test concludes that the individual on the right is likely to have reduced mineral reserves available, and consequently a higher acid level may be anticipated within the body tissues. The sharp rise in pH on the individual’s test to the left may apparently also reflect ammonia imbalances and is also worthy of further study. Important nuances in the test do exist and they are worthy of further research; Dr. Weatherby’s book may be helpful in this regard. | ||
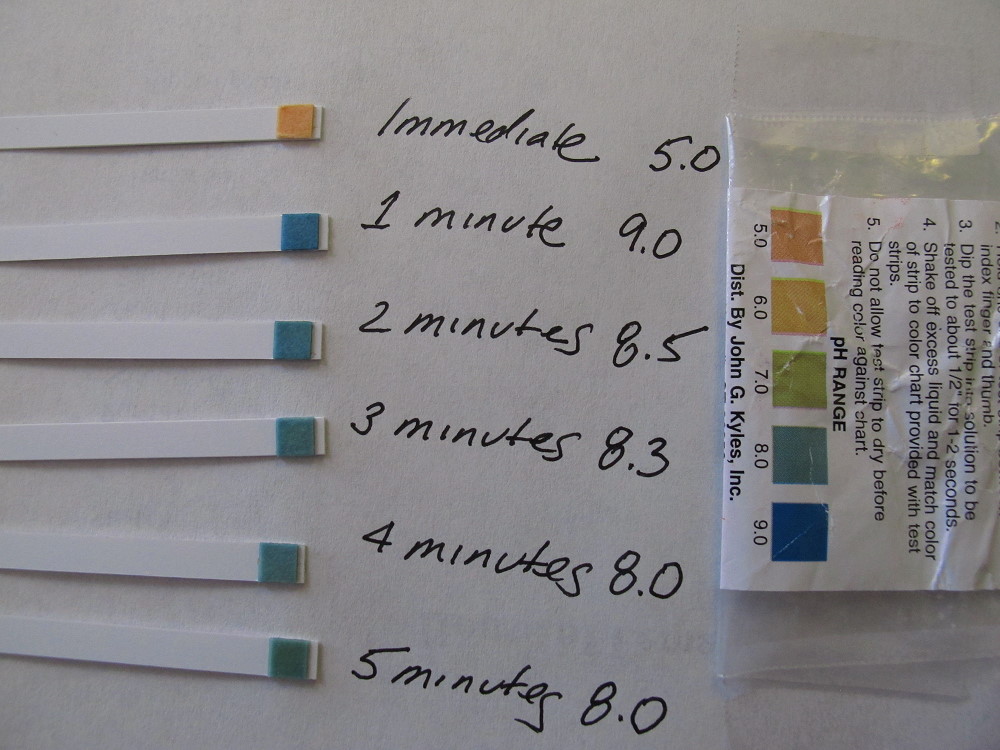
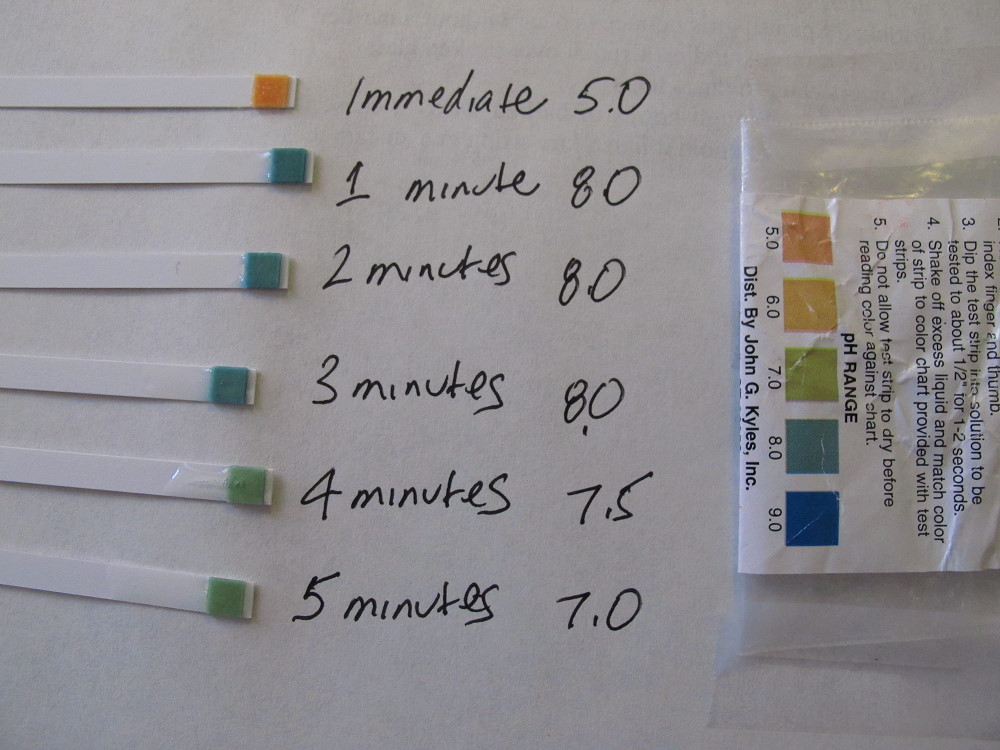
Additional simple tests for an acid-alkaline imbalance (i.e., breath holding test and respiratory rate test) are described in one of several of Dr. Dicken Weatherby’s books110b on the subject of functional medicine.
Any readers with a further interest in these topics may wish to consult those that practice in the field of functional medicine, or as stated repeatedly, the health practitioners of choice.
A general introduction to the fundamental principles and philosophy of functional medicine is available courtesy of Dr. Mark Hyman:

Listen to a more extended discussion by Dr. Hyman on the state of health and Functional Medicine.
We can speak of such issues of oxygen, energy, oxidation, acidity and pH at length, but me must move on to make further progress. For those that continue to profess that there are no relationships of consequence between these factors, or little that can be done about them, let us make a more blunt parting observation as to what happens in the body when we die. On the topic of acidosis (i.e., excessive acidity within the tissues), under the subtopic of associations, we learn starkly that111:
| “Lactic acidosis is an underlying process of rigor mortis. Tissue in the muscles of the deceased carry out anaerobic metabolism in the absence of oxygen, using muscle glycogen as the energy source, and significant amounts of lactic acid are released into the muscle tissue. With depletion of muscle glycogen, the loss of ATP [i.e., energy production]causes the muscles to grow stiff, as the actin-myosin bonds cannot be released. (Rigor is later resolved by enzymatic breakdown of the myofibers.) In meat-producing animals, the post-mortem pH drop in muscle tissue contributes to meat quality (by influencing water retention, cutting color and texture of meat) and also contributes to food safety by inhibiting several acid-intolerant spoilage organisms that otherwise might proliferate, even at refrigerator temperature.” |
It would seem as though there are obvious relationships that exist between acidity, oxygen, and energy production when we are dead. There is every reason to think that such relationhips exist while we live as well.
One famous line from mutated history and the cinema is that, “Today is a good day to die…”
Our alternative line for today (not quite so famous) is that, “It is a good time to talk about the thyroid.” And so on we go…
We can now recall the importance of the thyroxine, the primary hormone of the thyroid:
| “Thyroxine stimulates the production of oxygen in the body. Thyroxine is directly related to carbohydrate metabolism, protein synthesis and breakdown. Thyroxine stimulates the utilization of energy. Thyroxine directly affects the basal metabolic rate. Thyroxine stimulates the cells of the nervous system. Thyroxine is used to maintain the state of the cardiovascular system. Thyroxine stimulates the breakdown of fats. Thyroxine stimulates normal growth and development. Thyroxine stimulates the muscles to break down proteins. The thyroid is, therefore, a master regulator of metabolism for the body and any interference in that functioning is inevitably and seriously detrimental to human health.” |
We can see that the thyroid is the metabolic master of our system, and it is harder to get much closer to home than that. We also have good reason to suspect that thryroid processes are being interfered with in conjunction with the Morgellons condition. Our most fundamental indicator of this disturbance is that of body temperature. There is good reason as well as evidence to show that the body temperature of the general population is operating frequently at a temperature less than normal. The mantra of “98.6” that many of us grew up with may not exactly be quite so vocal these days, and the mystery of that silence is deserving of intensive study.
We also have reason to consider interference from the standpoint of aromatic chemistry; this has been discussed at length earlier in this paper. Essentially, the existence of aromatics along with amines is a perfect setup to initiate the halogenation of the aromatic structure. Halogenation of an aromatic structure by the halogens foreign to the body, e.g., fluorine, chlorine and bromine, is also the perfect setup to interfere with thyroxine, or the thyroid itself.
Third, we have a relationship of interference to consider between tyrosine (an amino acid), the thyroid (with thryoxine production) and dopamine (a neurotransmitter), as it has been discussed previously. We will also revisit this topic when the subject of neural disruption is discussed later. No matter which way go about it, we obviously have important issues at hand here, and metabolism and body temperature indicators are the heart of it. We will focus on this issue of body temperature, as it is direct and apparent, and it is easy to measure, and monitor for change. It is a macro indicator that affects the entire body system. Our Biochemistry is essentially non-functional without the proper conditions of temperature and pH in place (for ALL reactions), and we must never lose sight of this fundamental fact as we wade through this maze of complexity and interaction.
What does low body temperature mean, at the most fundamental level? It means the body is not working up to speed; the engine is not running at the proper temperature. If the engine does not run at the proper temperature we have incomplete combustion and less energy is produced. In essence, the body is not working as it should, and it is definitely not firing on all cylinders. In more conventional terms, an underactive thyroid is called hypothyroidism and the overactive thyroid is called hyperthyroidism. The signs of research in place point quite strongly to the former in association with the Morgellons condition.
Let’s look at the connection between temperature, metabolism and the thryroid from several sources and in more detail: First, a direct statement of the relationship from a detailed source on medical testing112:
|
“There is a direct link between low body temperature and low thyroid function. In fact, one of the symptoms of hypothyroidism is the reduction in body temperature.” |
In equal plainspeak, Dr. Rind introduces us to the importance of the relationship, as well as the role the adrenals have with respect to temperature variations113:
|
“If you’re not feeling quite up to par, take your temperature. Not to determine if you’ve got a fever – rather, temperatures reflect an individual’s metabolic energy state. The average daytime temperature of a healthy individual is 98.6 thus making 98.6 the optimal (as opposed to normal*) temperature. Lower than optimal temperatures reflect a lower than optimal metabolic state which is usually controlled by the thyroid mechanism. Wide variability of temperature reflects an unstable or fatigued adrenal system [please note this addition to our considerations -CEC]. Thus, on the road to health, one wants to go from low and/or unstable temperatures to 98.6 and stable if possible.” |
|
Detailed information about a method to monitor your temperature and its variability is available on Dr. Rind’s site as well. The awareness of the state of temperature in the body, its importance to efficient metabolism, and a system to track and monitor temperature on a regular basis may be a beneficial first step in becoming aware of the importance of thyroid functioning to good health. |
Lastly, to cement the importance of the relationship of body temperature to thyroid functioning, Dr. Weatherby also describes a Body Basal Temperature Test114 and reiterates the primary point made:
|
“A reduced core body temperature is one of the hallmarks of thyroid hormone deficiency and hypothyroidism.” |
The widespread reporting and observation of reduced body temperature amongst the general population , in addition those those more visibly suffering from the Morgellons’s condition, should make it apparent that hypothyroidism is a central topic of research here. This paper can only hope to introduce the importance of this issue in this and future studies..
If we postulate that a state of hypothyroidism exists, i.e, a state of lowered metabolic rate associated with the lower body temperature cited above, what then are some of strategies offered by the health community to alter this situation? It would certainly seem, then, that the cause of such a problem would need to be identified first. We have certainly called attention in this paper to the possible role that the halogens might assume in such a case, and the interference that the toxic halogens can create. An obvious first approach might be to reduce or eliminate the presence of toxic halogens within the body, and to avoid contact or ingestion of them. Let us seek out how the health communities might react this to this potential problem.
If we begin by asking the question of how one would detoxify from an excess of halogens, especially that of fluoride and bromide, we are immediately led to an abundance of discussion related to iodine therapy. The reasons for this have already been discussed, and these relate to the relative reactivity of the halogens and their competition of iodine within the thyroid. We can repeat that relationship with the words, to start, from Dr. Mark Sircus :115
|
“It is well known that the toxic halides, fluoride and bromide, having structure similar to iodine, can competitively inhibit iodine absorption and binding in the body.” |
We are also immediately led, therefore, to a strategy of great importance and interest, i.e., iodine therapy, or the intake of additional iodine into the body. Expressed as follows by Dr. Sircus in conjunction with Dr. Gyula:
|
“Iodine intake immediately increases the excretion of bromide, fluoride, and some heavy metals including mercury and lead. Bromide and fluoride are not removed by any other chelator or detoxifying technique. Dr. Kenezy Gyula Korhaz states that iodine chelates heavy metals such as mercury, lead, cadmium and aluminum and halogens such as fluoride and bromide, thus decreasing their iodine inhibiting effects especially of the halogens.“I |
It is more than explicit at this point that no medical advice is ever given or implied within these papers, however, information and education IS to be freely available to all. It is clear from the literature and research that iodine supplementation in connection with thyroid performance is extensively discussed and employed. The chemical and molecular rationale for that strategy has already been made clear within this paper; the details of consideration and application will be left to the reader. The responsibility for education and professional consultation in any such matters is also equally obvious.
Examples of the need for education and consultation on the matter is apparent from the following two complicating factors:
1. Another strategy, commonly employed, is that of prescribing an increase in the thyroid hormone (T4) itself to remedy hypothyroid (decreased thyroid function) imbalances. In the book, Thyroid Balance, by Dr. Glenn Rothfeld, we read that:116
|
“Doctors typically prescribe a thyroid supplement -a drug that boosts the thyroid hormones in your system -to treat most thyroid imbalance. This is a tried-and-true therapy that has been the standard for more than a century. The earliest documented use of this therapy dates to 1891, when doctors started using ground thyroid gland tissue from sheep to treat severe hypothyroidism” |
2. Allergic reactions to iodine supplementation are known to exist. The extent and reaction of an allergic reaction is certainly outside the scope of this article, but attention will at least be drawn to the matter.
3. Another question that can be asked, similar to those issues that were raised earlier with respect to deficiencies in iron, is whether or not we take care of a deficiency by simply adding more of the same thing back into the system? If we do not understand what is causing the deficiency of a particular substance to begin with, supplementing it with the same substance may be a completely futile exercise. Hence the interest of “Thyroid Inhibition” increases, and consequently the interplay with iodine remains a focal point of the strategies discussed here.
4. The relationship between adrenal performance (and cortisol levels) and thyroid function is also important to be aware of. There is some information from the research of this Institute that the undue stresses on the adrenal glands may well be another point of serious research as it relates to the Morgellons condition. There is an additional caution provided to us for the simplistic response of simply increasing the thyroid hormones with supplements:117
|
“Thus, it can be important for you and your doctor to rule out insufficient adrenal function before raising too high on natural dessicated thyroid or T3…” |
Self-tests for adrenal function are subsequently described in this article, but the point is again made that thyroid hormone supplementation may be a diversionary exercise.
Education and research are the goals here, not therapy. Education and research are obviously on the path toward therapy, and these are our pursuits.
While we are on the subject of self-tests, let us include another test, this time related to iodine deficiency. There is an additional test entitled the Iodine Patch Test within Dr. Weatheryby’s book mentioned earlier118. It is a simple test that monitors the fading of an iodine patch (2%) painted onto the skin over a 24 hour period. As Dr. Weatherby describes,
|
“The Iodine Patch Test is an excellent test for assessing for iodine deficiency…Unfortunately, iodine deficiency is widespread because of the prevalence of chemicals such as chlorine, bromine and fluoride [note halogen emphasis – CEC] in our environment and water supply. These chemicals will quickly deplete iodine from the body and interfere with iodine metabolism leading to a number of problems including hypothyroidism, lowered vitality, cognitive dysfunction, lowered immunity, and obesity. The iodine patch test is an easy method of assessing your iodine levels.“ |
Once again, we may ask, does this sound familiar, relevant and germane to the findings of this report?
Readers are referred to Dr. Weatherby and other sources for more particular details on the interpretation of the test results. There are those who think that the iodine patch test is not reliable and therefore not useful; as such it exists in controversy amongst some practitioners.119 It would appear that the lower body temperature test is less so and it is simple in principle to comprehend. Recall from earlier discussions that all biochemical reactions take place at a specific temperature and pH; alteration of either of these parameters will inevitably lead to impairment of some sort or fashion.
We start this by mentioning forms that are not advisable and that have varying levels of toxicity – conventional antiseptic iodines. The first clue that such forms are not of benefit is the warning label, which will clearly state that this form is not to be used for internal purposes. There are two forms described that are in common use:120, 121
1. Tincture of iodine – a mixture of elemental iodine and either potassium or sodium iodide, dissolved in ethanol and water Denaturing of the alcohol is also know to be used in commercial tinctures. A 2% free iodine solution contains about 1 mg of free iodine per drop. Ethanol is poisonous in sufficient amounts and denatured ethanol is deliberately poisoned to prevent consumption. Tincture solutions can vary between 2% – 7% in strength.
2. Povidone iodine is a mixture of PVP (polyvinylpyrrolidone) and elemental iodine. It is soluble in both water and alcohols, and is more stable chemically than tincture of iodine. The deposition of PVP in human tissues reported in toxicology tests warrants abstention from use internally.122
We now transition to forms that are more suitable internally to the body (notwithstanding the prior caveats of potential allergic reactions, etc.). A statement of additional risk factors associated with the ingestion of iodine are included from the following medical bulletin from the National Institutes of Health; all readers are advised to be aware of all information that is contained within this report.123
Medline Plus : Iodine :
(http://www.nlm.nih.gov/medlineplus/druginfo/natural/35.html)
Now that we have given due notice to the federal standards for recommended levels of iodine in the body, let us open up the discussion to various professionals that have devoted significant study to iodine as it relates to health. It will be clear that the federal recommended levels are dramatically at odds with many serious research studies on the subject. For an extended discussion and debate between those at the forefront of iodine therapies (Abraham, Brownstein) and those advocating more restrictive conventional approaches (Gaby), please see the following paper:124
The following media presentations are recommended as an introduction to the important role that sufficient iodine and iodide levels plays with in our health. More extended discussions of the necessary levels of iodine in the body, the manufacture and storage of iodine, differences between iodine and iodine forms, body capacity and removal of excess iodine, skin issues related to iodine deficiency, the damage and competition for iodine by the halogens, the dangers of the halogens with respect to modern diets, and improved brain functioning with appropriate iodine levels are all important topics that are covered in these presentations. The reader is advised to become familiar with the material that follows.
(Here is a test for you: find the place in one of the videos where “RDA” is stated to stand for a “really dumb idea (sic?)”.)
Jorge Flechas, MD, on the topic of Iodine Sufficiency
Dr. Brownstein, MD, Iodine, the most misunderstood nutrient
Drs. Mercola & Brownstein, MD, on the topic of Iodine Deficiency
(note the attention given to the bromine issue)
Dr. Tenpenny, on the topic of Iodine Deficiency
(Advanced Discussion)
We can see from the presentations by numerous doctors and extensive research that there is a strong case for the existence of increased levels of toxic halogens in the body (i.e., fluorine, chlorine and bromine) and for the competition that they exert upon iodine and the thyroid. This case in in alignment with the spectral and biochemical analyses that are a core result of this paper.The symptoms of impaired thyroid function such as reduced body metabolism and energy production, lowered body temperature, skin complications, brain dysfunction, cancers and many other serious health issues are intimately related to iodine deficiency. Iodine therapies are also offered as a significant prospect for improvement by these same doctors. The case for the existence of the aromatic halogens in association with the Morgellons condition has also been made by this researcher through the use of infrared spectral analysis, with a particular interest in bromine substitutions. It is also important to emphasize the major differences in the amounts of iodine that are necessary and utilized in the body compared to those identified in the federal standards; this difference ignores the prospect of increased competing halogen sources that may now have been introduced into the body. This difference, even based upon conventional medical research of recent decades as outlined in the presentations above, is on the order of 100 times. Impairment of thyroid functioning and iodine supplementation therapies exist, therefore, as compelling and major topics of further research in the investigation of the Morgellons condition.
We now begin to close this chapter of research in the history of Carnicom Institute, and we depart (temporarily, of course) with a brief revisit to, and a discussion of, the neural disruption issue. It is difficult to ‘rank’ the relative importance of the numerous issues that have evolved within this current research and their combination is devastating and ostracizing to far too many. This level of harm and suffering is much greater than that which is currently acknowledged, and many individuals deserve recognition for the battles they are fighting. These battles are often fought in solitude and they can be literally a fight for life itself. We must offer our compassion, our care and our help in haste, as the frog pot continues to warm for most of us.
It is clear that cognitive functioning, concentration ability and mental acuity in general are companions of study here, and that they are closer to home than many of us would like to admit in our pursuit of improved health.
The technical and evidentiary argument for this situation has already been made in this report, and our question here is what can be offered as a prospect for improvement? Certainly the first fact to recognize is that the broad health impacts that have been discussed here are usually related to one another, and it is simplistic to separate them as islands of trouble. How can we possibly suspect a simple ‘cure’ to any demise of neural and cognitive functioning; in the majority of cases modern medicine is still in its infancy here. Nonetheless, there are ALWAYS paths to pursue to improve the lot of us, and there are no exceptions here.
We may start with the glaring theme of oxidative stress, which is pervasive and illustrative of the connections between the topics of this report and those that are at the foundation of pathology. This foundation (e.g., Robbins125) has already been discussed some time ago in a context that is much broader than the Morgellons issue by itself. Is it any surprise when we learn, therefore, that:126
|
“Oxidative stress plays a pivotal role in the pathogenesis of neurological disorders.” |
and, in the discussion of a professional textbook on the subject, that127:
|
“The role of free radicals and oxidative stress in neurological disorders has only recently been recognized… Oxidative Stress and Free Radical Damage in Neurology sets the record straight, focusing on clinical and research issues regarding the interplay of free radicals and the human nervous system. Crucially, the chapters cover numerous antioxidants and their possible therapeutic role in neurological disorders. Key illnesses such as epilepsy, multiple sclerosis and Parkinson’s are analyzed, and chapters also examine more general issues such as the link between free radicals and inflammation of the central nervous system..” |
And again, to eliminate any doubts on relevance128:
|
“It has been demonstrated that oxidative stress has a ubiquitous role in neurodegenerative diseases.” |
We see the consequences of oxidative stress over and over, and at this point we are not entitled to remain ignorant of what we can and must do to improve the situation. The details and important role that anti-oxidants play in combating oxidative stress have been repeatedly emphasized in this report. We must take advantage of that same information here as it relates to neurological functioning.
We have also introduced leading research on the importance of glutathione as it relates to neurological diseases and Parkinson’s disease. It should be recognized that glutathione is one of the most powerful antioxidants known, and from the above, it should come as no surprise to us that its effectiveness against oxidative stress is important to neural functioning. The importance of understanding the precursors of glutathione (e.g., N-acetyl cysteine (NAC) and alpha lipoic acid) vs. dietary supplemention or ingestion has also emphasized in this paper.
Through the introduction of iodine therapies that are practiced to improve the functioning of the thyroid, we have also learned that adequate levels of iodine are also strongly related to mental functioning, acuity and intelligence. This topic is especially prominent in the presentation by Jorge Flechas, MD, above. We have also learned that the difference between the federal guidelines of minimum daily iodine levels and the levels deemed beneficial by certain medical practitioners is dramatic, to say the least. This dosage issue is entirely independent from any need to compensate for the potential reduction or removal of iodine stores within the body by competing aromatic halogen compounds (as they have been identified and postulated within this report).
We have also called strong attention to the intriguing and serious implications of oxydopamine and its related compounds within this growth form. There is a strong case in the data of this report for this type of existence, and the damage that these compounds have upon neurological function is unambiguous. Recall that such compounds are used in the laboratory to deliberately induce Parkinson’s Disease. Such compounds reduce dopamine and brain amine levels and this, as a minimum, is known to affect memory loss and cognitive functioning.
With respect to the potential mitigation from this effect, oxidative stress is responsible for dopamine loss129, so this is now a familiar refrain to us. The role of antioxidants has been discussed at length in this report, and this presents the roles and use of vitamins (e.g, A, B, C, D, E), enzymes, and the precursors to glutathione for example.
Readers and health practitioners will also want to investigate the role of tyrosine and L-tyrosine as they relate to dopamine levels in the brain. Tyrosine is an amino acid, and it is the building block for dopamine as it has been discussed. The prospect of structural interference in the synthesis of dopamine has also been raised within this report, especially with prospect of halogen substitutions on the aromatic ring of tyrosine.
The role of diet and nutrition is also important to dopamine levels.130 I am hoping that it is now understood, from the journey that has been shared, that this researcher advocates nutrition as one of the primary pathways towards better health, and that those who are knowledgeable in such ways deserve our greater recognition and attention. They have been driven to the heart of the matter, and that is that all life will eventually be a product of the nourishment that it consumes. The business of “supplementation” is essentially a band-aid to attempt to compensate for a deficiency that never should have existed if we were wiser and more complete in our ways, especially from youth onwards.
While we are on the subject of nutrition, a specific nutritional drink recipe is available on this site. This recipe is a culmination of health research by Carol Carnicom over a period of several years and it now also combines many of the important research findings from the study of the Morgellons condition. It is a nutritional approach to some of the needs that have been established, therefore, from a variety of perspectives. Protein sources, joint issues, iron utilization and the need for iodine are each examples of the ties that have evolved over the years between research and nutrition. The reader may find this information to be of value in some unexpected ways, and I encourage you to become familiar with both its pleasures and its constitution. The link to ”Carol’s Smoothie Recipe” follows below:
“Carol’s Smoothie Recipe”
(.pdf download)
Continuing on the subjects of neural, mental and cognitive functioning, some of the food sources that are known to benefit tyrosine and dopamine levels include, therefore131,
|
“Foods highest in L-tyrosine include: Fava beans Duck Chicken Ricotta cheese Oatmeal, Mustard greens Edamame Dark chocolate [Now, there’s an excuse…-CEC] Seaweed Wheat germ ” |
The role of diet, nutrition and enzmyes in improved neural functioning is also discussed at length in the following report from the U.S. Department of Agriculture, entitled “Nutrition and Brain Function”. We learn here again the important role that antioxidants play with the summary statement that:132
|
“Perhaps there is no better place in which to gauge the power of antioxidants than between the minute connections of the nerve cells.” |
Two additional points of interest are also mentioned in this report. The first is the recognized benefits of enzymes (specifically, ‘kinase” enzymes) to brain functioning. Notice also that even though the size of the brain is quite small relative to the body, it ends up using significant amounts of oxygen during mental activity. The availability of sufficient oxygen and body’s ability to use this oxygen effectively are obviously of importance here. We see once again that it is a hopeless exercise to seek out singular causes, effects and ‘cures’ to the complex health problems before us, and the joint appearance of antioxidants and enzymes in the crusade against oxidative stress has again made its mark here.
Another word of importance within this paper concerns the regeneration of brain neuron cells, termed “neurogenesis”. This work shows that adages die slowly, and that it is only recently accepted in the mainstream scientific community that the brain is not a fixed organ which can only deteriorate with age. The research shows that brain neurons can be regenerated, albeit at a slower rate, at more advanced ages with proper nutrition. This means “new” brain functioning and development can continue in the aging process and that “disease” is not a fixed sentence. One must be careful of old adages, lest we become fixed ourselves in our ways, thinking methods and perceptions.
Additional well known natural approaches to improve mental clarity and function include those of Gingko Biloba and CoQ10. Whether or not these particular supplements will be of known benefit with the Morgellons situation remains to be seen; they have, however, established reputations with respect to improving mental clarity and memory loss. The following paper133 discusses a series of natural remedies to enhance memory and mental function, and it is anticipated that they may be of some benefit.
Enhancing Memory and Mental Functioning – NYU Langone Medical Center
It is a primary argument of this researcher that the solution to a problem is not necessarily found by introducing additional complexity into the situation. The case for “supplementation” of diet to compensate for health problems is a primary example of this dilemma. If one has known sources for health problems, it is usually wiser to eliminate the source of the problem rather than try to compensate for it with an infinite combination of variables, such as pills, supplements, or drugs, for that matter. The proper approach for the “Morgellons” condition, as with any health impairment or “disease” is to strike to the source of the matter. If the cause or source of such a condition can be identified, it is to be removed or stopped in its tracks, if at all possible. It is not be be accepted as intrinsic to the environment and then compensated for with a myriad of protocols, drugs, treatments, and supplements in a state of perpetual uncertainty and ignorance. A body of information is available to those who wish to seek it out, and this information (along with your participation) can be a pathway towards striking at that source of health and disease. The general population, the health communities, the professional communites, and the governmental structures are obligated, as has been stated repeatedly, to combine, use and express their knowledge and talents to improve the state of the environment and the health of the people. We, our children, and our future children deserve no less than this, and the entire world deserves the more of it.
This episode of research now comes to a close; this paper has taken more than a year to complete and additional needs remain before us. Additional work will be done in the future to summarize and consolidate the essentials of this research. Work of this nature is a journey in itself, and I do not know where it will lead and end when I start. The process of identification, correlation and analysis has now taken place, and it is hopeful that it provides a beneficial foundation from which we may accomplish greater things in the future. I thank you for your patience and endurance to reach these closing comments and I hope that the work has been of value to the general readership. The future remains to be influenced by the decisions and actions that we now take together.
Sincerely,
Clifford E Carnicom
(born Clifford Bruce Stewart, Jan 19 1953).
Additional Note:
Appreciation is extended to Lucretia Smith and Dr. Jimmie McClure for their sustained interest, research and communication to CI over a period of several years about the importance and relevance of thyroid issues to the work presented here. These individuals, along with others, deserve credit for their prescient assessments of the role that thyroid dysfunction is likely to play in the “Morgellons” condition. Many thanks to both of you.
Sincerely,
Clifford E Carnicom
END OF PART III
References:
1. Infrared Absorption Spectroscopy – Practical, Koji Nakanishi, Holden-Day, Inc., 1962.
2. Reprint of Colthrup Chart of Characteristic Group Absorptions in Modern Methods of Chemical Analysis, Robert L. Pecsok, John Wiley & Sons, 1976.
3. IR Pal Software 2.0, Dr. Wolf van Heeswjik, 2010, Wolf’s Shareware and Freeware,
4. Spectral Database for Organic Compounds (SDBS), National Association of Advanced Industrial Science and Technology (AIST), Japan.
5. Biochemistry, John T. Moore, Wiley Publishing, 2008.
6. Organic Chemistry, John McMurry, Brooks/Cole, 2004.
7. Ibid., McMurray.
8. Oxford Dictionary of Science, Oxford University Press, 1999.
9. Organic Chemistry, Bruce A. Hathaway, Ph.D., Barron’s, 2006.
10. Biochemistry, John T. Moore, Wiley Publishing, 2008.
11. Chemistry, The Central Science, Theodore L. Brown, Pearson Prentice-Hall, 2006.
12. Ibid., Moore.
13. Ibid., Hathaway.
14. Ibid., Oxford.
15. Ibid., Brown.
16. Ibid., McMurray.
17. Ibid., Oxford.
18. Ibid., McMurray.
19. Principles of Biochemistry, H. Robert Horton, Prentice Hall, 1993.
20. Ibid., Oxford.
21. Ibid., McMurray.
22. Ibid., Hathaway.
23. Ibid., Oxford.
24, 25. Ibid., McMurray.
26. Ibid., Oxford
27. Ibid., McMurry
28. Ibid., Oxford.
29. Morgellons : A Thesis, Clifford E Carnicom, Oct 2011, www.carnicominstitute.org.
30. Morgellons Research Project : Scientific Study of the Morgellons Condition, Carnicom Institute.
31. Free Radicals in Biology and Medicine, Dr. P.K. Joseph
32. Iron Deficiency, Wikipedia, wikipedia.org.
33. Amino Acids Verified, Clifford E Carnicom, Nov 2012, www.carnicominstitute.org
34. Amino Acid Chart, Dr. Guy Wilson, www.1choicevitamins.com.
35. Ibid., McMurray.
36. Principles of Biochemistry, Albert L. Lehninger, Worth Publishers, 1982.
37. ATSDR – Medical Management Guidelines : aniline, U.S. Department of Health and Human Services, CDC.
38. Wikipedia.org
39. Effects of Acidity, Dr. Michael Lam
40. pH Balance and Your Health, wellnesswatchersmd.com
40b. The Acid Alkaline Food Guide, Dr. Susan E. Brown, Square One Publishers, 2006.
41. Are Your Teeth at Risk, www.docprior.com
42. Robbins Pathological Basis of Disease, Ramzi S. Cotran, M.D., W.B. Saunders Company, 4th Edition, 1989.
43. Biochemistry Demystified, Sharon Walker, Ph.D., McGraw Hill, 2008.
44. Ibid., McMurray
45. Ibid., Morgellons : A Thesis, Carnicom
46. Aromatic Substitution Reactions Part II, www2.chemistry.msu.edu
47. General Discussion of Common Mechanisms for Aromatic Amines, IARC.4
48. Oxidopamine, wikipedia.org
49. Hazardous Materials Chemistry for Emergency Responders, Second Edition, Robert Burke, CRC Press, 2003.
50. Hepatotoxicity and mechanism of action of haloalkanes: carbon tetrachloride as a toxicological model., BioInfoBank Library, Critical Reviews in Toxicology, Nov 29, 2012.
51. Mechanism of Anesthetic Toxicity: Metabolism, Reactive Oxygen Species, Oxidative Stress, and Electron Transfer, ISRN Anesthesiology Volume 2011.
52. Organometallic Compounds, Michigan State University, Department of Chemistry, msu.edu.
53. Halogens & Their Compounds: Health Hazards, International Labor Union, www.ilo.org
54. Spectral Database for Organic Compounds (SDBS), National Institute of Advanced Industrial Science and Technology (AIST), Japan
55. Effect of 6-hydroxydopamine on brain norepinephrine and dopamine: Evidence for selective degeneration of catecholamine neurons, George R. Breese, National Institutes of Health.
56. Desipramine attenuates working memory impairments induced by partial loss of catecholamines in the rat medial prefrontal cortex, SM Clinton, National Institutes of Health.
57. Ibid., Cotran.
58. Ibid., Cotran.
59. Morgellons : In the Laboratory, Clifford E Carnicom, May 2011, www.carnicominstitute.org.
60. Morgellons, The Breaking of Bonds and the Reduction of Iron, Clifford E Carnicom, Nov 2012, www.carnicominstitute.org
61. Ibid., Morgellons : A Thesis, Carnicom
62. Risks of Iron Supplements, www.livestrong.com
63. Ibid., Risk of Iron Supplements
64.The role of vitamin C in iron absorption, L. Hallberg, National Institutes of Health.
65. Ibid, Morgellons, The Breaking of Bonds and the Reduction of Iron, Carnicom.
66. Ibid., Morgellons : A Thesis, Carnicom
67. Ibid., Amino Acids Verified, Carnicom.
68. N-acetylcysteine (NAC), David Wheldon.
69. A Mechanism of Blood Damage, Clifford E Carnicom, Dec. 2009, www.carnicominstitute.org
70. Ibid., Morgellons : A Thesis, Carnicom
71. Ibid., Morgellons : A Thesis, Carnicom
72. Ibid., A Discovery and A Proposal, Clifford E Carnicom, Feb. 2010, www.carnicominstitute.org.
73. Ibid., Cotran.
74. Ibid., A Discovery and A Proposal, Carnicom.
75. Free radicals, antioxidants, and human disease curiosity, cause, or consequence?, Barry Halliwell, Lancet, Sept 10, 1994 v344 n8924 p721(4), published at auraresearch.com.
76. Ibid., Cotran.
77. Oxidative Stress and Neurodegenerative Diseases: A Review of Upstream and Downstream Antioxidant Therapeutic Options, Current Neuropharmacology, Mar. 2009, Bayani Utara, National Institutes of Health.
78. Free Radicals, Oxidative Stress, and Diseases, Enrique Cadenas, MD PhD, Professor of Pharmacology, University of Southern California.
79. Alcohol, Oxidative Stress and Free Radical Damage, Defeng Wu, PhD, Alcohol Research & Health, National Institues of Health.
80. Ibid., A Discovery and A Proposal, Carnicom
81. Ibid., Cotran.
82. Ibid., Cadenas.
83.Ibid., Cadenas.
84. Structure and reactivity of radical species, University of California at Davis., www.chemwiki.ucdavis.edu
85. Diradical Chemistry, The Chemogenesis., www.meta-synthesis.com
86. Magnetic Liquid Oxygen, University of Illionois, Chemistry Department.
87.The Balancing of Oxidants and Antioxidants, Pharmaceutical Field, www.pharmafield.co.uk
88. Ibid., Cadenas.
89. Ibid., Pharmaceutical Field.
90. Ibid., Pharmaceutical Field.
91. Ibid., Pharmaceutical Field.
92. Free Radicals and Reactive Oxygen, Colorado State University, Biomedical Hypertexts.
93. Ibid., Colorado State University.
94. Ibid., Morgellons, The Breaking of Bonds and the Reduction of Iron, Carnicom.
95. Morgellon’s : The Role of Atmospheric Aerosolized Biological Nano-Particulates, An Anonymous Physician.
96. Ibid., Morgellons, The Breaking of Bonds and the Reduction of Iron, Carnicom.
96b. Oxidata Test, www.oxidata.com
96c. Free Radical Urine Test, www.naturalchoicesforyou.com
96d. How Do Anioxidants Work Anyway?, Kristy Russ, www.antioxidants-make-you-healthy.com
97. Wikipedia.
98. Ibid., Wikipedia
99. Understanding Urine Tests, National Institutes of Health, www.nih.com
100. Acidic Body, Michael Lam MD, www.drlam.com
101. Acid Base Balance in Critical Care Medicine, Patrick J Neligan, Clifford S Deutschman, Patrick Neligan Deparment of Anesthesia, Univ. of Pennsylvania, 2005.
102. Acid-Base Tutorial, Dr. Alan Ggrogono, , www.acid-base.com.
103. Ibid., A Discovery and A Proposal, Carnicom, Feb. 2010.
104. Morgellons : Growth Inhibition Confirmed, Clifford E Carnicom, Mar 2010, www.carnicominstitute.org.
105. Ibid., Morgellons : A Thesis, Carnicom
106. Alkaline Water and Why Avoid It, Lawrence Wilson, MD, Center for Development, Inc., www.drwilson.com.
107. Sugars and dental caries, Riva Touger, The American Journal of Clinical Nutrition.
108. Urine and Saliva pH Testing, Michael Biamonte, C.C.N, www.health-truth.com
109. In Office Lab Testing : Functional Terrain Analysis, Dr. Dicken Weatherby, www.bloodchemistryanalysis.com.
110. Dr. Henry G. Bieler, Wikipedia.
110b. Complete Practitioner’s Guide to Take-Home Testing : Tools for Gathering More Valuable Patient Data, Dr. Dicken Weatherby, www.bloodchemistryanalysis.com.
111. Lactic Acidosis, Wikipedia.
112.Relation Between Low Body Temperature and Thyroid, www.medicalhealthtests.com
113. Metabolic Temperature Graph, Bruce Rind M.D., www.drrind.com.
114. Ibid, Weatherby.
115. Iodine and Detoxification, Dr. Mark Sircus., www.drsircus.com
116. Thyroid Balance, Dr. Glenn Rothfeld, MD, Amaranth, 2003.
117. How Adrenals Can Wreak Havoc, www.stopthethyroidmadness.com.
118. Ibid., Weatherby.
119. Unconventional Tests and Procedures to Diagnose Thyroid Diseases, www.thyroid.about.com
120. Tincture of Iodine, Wikipedia
121. Povidone Iodine, Wikipedia
122. Toxicity Profile, Polyvinylpyrrolidone, legacy.library.ucsf.edu.
123. Medline Plus : Iodine, National Institutes of Health
124. The Great Iodine Debate, www.westonaprice.org
125. Ibid., Cotran.
126. Oxidative stress and neurological disorders in relation to blood lead levels in children, M Ahamed, National Institutes of Health.
127. Naton Gadoth, Oxidative Stress and Free Radical Damage in Neurology, Springer, 2011.
128. Oxidative Stress in Neurodegeneration, Varsha Shukla, Hindawi Publishing Corporation, 2011.
129. Katlid Rahman, Studies on free radicals, antioxidants, and co-factors, National Institutes of Health.
130. Bryce Wylde, The Dopamine Diet, www.doctoroz.com.
131. Ibid., Wylde.
132.James A. Joseph, Nutrition and Brain Function, U.S. Department of Agriculture.
133. Enhancing Memory and Mental Functioning , NYU Langone Medical Center, www.med.nyu.edu.
